|
Almost every person from time to time gets a cold or even gets a more serious viral infection, gets vaccinated. But after some time after recovery, it begins to seem that the symptoms are returning - the patient feels a breakdown, aching joints, an increase in temperature. The danger is that these can be signs of a serious illness - Guillain-Barré syndrome, sometimes leading to complete paralysis and death. What is this disease and how to protect yourself from it?
General information
Guillain-Barré syndrome is an autoimmune lesion of the peripheral nervous system, in which muscle weakness can rapidly develop, turning into paralysis. Often it becomes the cause of acute flaccid tetraparesis, in which the motor activity of the lower and upper extremities decreases. In ICD-10, Guillain-Barré syndrome is designated by the code G61.0 and is included in the group of inflammatory polyneuropathies.
Guillain-Barré syndrome is an autoimmune lesion of the peripheral nervous system.
There are two types of GBS classification - according to the form of the disease and according to its severity. According to the first indicator, the following types of syndrome are distinguished:
- AIDP, also called acute inflammatory demyelinating polyneuropathy. This is the most common form - it affects from 65 to 90% of cases;
- acute axogonal neuropathies of a motor or motor-sensory nature affect from 5 to 20% of patients. Designated in medical practice OMAN and OMSAN, respectively;
- 2-3% get sick with Miller-Fisher syndrome, about the same number of people have a paragenetic form of GBS;
- less than 1% falls on such types as sensory, pharyngo-cervico-brachial and paraparetic.
According to the severity, the following categories can be distinguished:
- Easy, in which the patient does not experience difficulties in self-care. Muscle weakness is almost not expressed, the person walks by himself.
- Average - the patient cannot walk 5 meters without additional help, his motor functions are impaired, fatigue quickly sets in.
- Severe - the patient is no longer able to move, often cannot eat on his own and requires constant care.
- Extremely difficult when a person needs supporting life support.
The course of Guillain-Barré syndrome is divided into several stages of development:
- in the first, lasting 1-4 weeks, the symptoms increase until the acute period occurs;
- on the second, the disease proceeds smoothly, the patient in this state spends up to 4 weeks;
- the recovery period is the longest, it can last for several years. A person at this time comes back to normal and may even be completely cured.

Guillain-Barré Syndrome Can Be Cured
Causes of Guillain-Barré Syndrome
There is still no reliable information about why this ailment appears. In modern medicine, it is believed that the consequences of past infections, including respiratory, cytomegalovirus, herpes, lead to the disease, and a person can also get sick due to previous mononucleosis and enteritis. Doctors explain this by the fact that immune cells confuse tissues infected with viruses with nerve endings and seeks to destroy them.
Less commonly, the appearance of the syndrome is attributed to trauma (especially craniocerebral), complications after surgery, the influence of systemic lupus, malignant tumors or HIV.
Another risk group is made up of people with a hereditary predisposition. If your family has had the syndrome, then it is better to take care of yourself - avoid infections and injuries.
Other reasons are possible, but it is much more important not to determine where the disease came from, but to notice its first manifestations and start treatment on time.
Guillain-Barré syndrome symptoms
It is not easy to identify the first manifestations of GBS; at first, they are quite similar to the signs of acute infectious diseases. Specific indicators appear only at later stages. Typically, the initial symptoms of Guillain-Barré syndrome include:
- the temperature rises sharply to very high, sometimes subfebrile;
- goosebumps and tingling sensations are felt on the tips of the clubs;

One of the symptoms of the disease is a sharp rise in temperature.
- the patient feels pain in the muscles;
- over time, weakness appears, the patient loses strength.
As soon as you see these symptoms either in yourself or in someone close to you, see your doctor immediately. Every minute wasted increases the risk of paralysis and even death.
Complications associated with Guillain-Barré syndrome
The disease has a huge impact on the functioning of the human body. Its course may be associated with such disabilities:
- difficulty breathing and the lack of oxygen caused by them;
- pain and numbness in different parts of the body;
- disorders in the intestines and genitourinary system caused by weakening of smooth muscles;
- the formation of a large number of blood clots;
- heart problems and fluctuations in blood pressure;
- bed sores appear in bedridden patients.
For each of the complications, symptomatic treatment should be applied, aimed at improving the patient's condition and bringing the body back to normal.

Blood pressure fluctuations may appear
Manifestations of Guillain-Barré syndrome in children
Adults are more likely to develop GBS, especially after forty. In children, it occurs much less often, but is characterized by the same symptoms, supplemented by eye paralysis, the absence of some reflexes and incoherent muscle work. Guillain-Barré syndrome in children often does not cause fever, which complicates the diagnosis and leads to complications.
Diagnostics of the Guillain-Barré syndrome
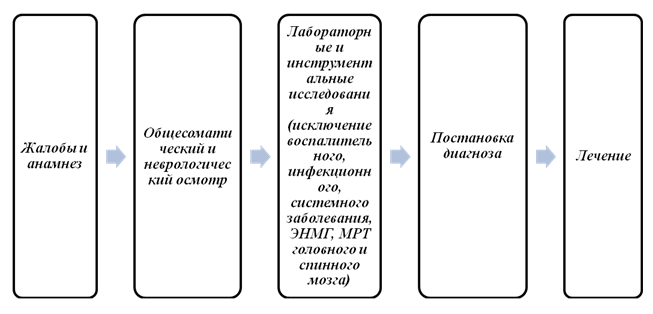
First of all, the doctor collects a complete anamnesis of the disease, while paying attention to both the presence or absence of causes of the disease, and the identified symptoms - the speed of their manifestation, the presence of pain and weakness, impaired sensitivity.
The next stage - a physical examination - should provide answers to questions about the patient's clarity of consciousness, the absence or decrease of reflexes, the presence of pain, autonomic problems. The lesions should be symmetrical and get worse over time.
At the third stage, laboratory tests are carried out. The patient donates blood for biochemical analysis, as well as for the presence of autoantibodies and antibodies to past diseases. A lumbar puncture is often done for general analysis of cerebrospinal fluid.

The patient needs to donate blood for biochemical analysis
Clinical guidelines for determining Guillain-Barré syndrome suggest instrumental diagnostics. The patient may be prescribed electromyography, which shows the speed of the signal moving along the nerves, and neurophysiological examination. It tests the work of the long nerves (sensory and motor) in the arms and legs. The survey is subject to at least four of both. The results of the two methods are compared, and a decision is made on the diagnosis.
Treatment of Guillain-Barré syndrome
There are two different systems of therapy that complement each other perfectly - symptomatic and specific. The first is to remove the consequences of the disease for the body - to help digestion, care for the body and eyes, support breathing, and control the work of the heart. Such care should protect the patient from further deterioration and complications.
Specific therapy should help the patient return to normal. There are several methods:
- Treatment of Guillain-Barré syndrome with the introduction of immunoglobulin into a vein. This drug is especially important for those patients who cannot walk.
- Plasmapheresis can speed up recovery in moderate and severe disease. For an easy form, it is not relevant. Removal of large amounts of plasma helps to normalize immune functions.
An important nuance - in no case should you combine both types of therapy for simultaneous use, as this can give unpredictable and dangerous results.

Plasmapheresis in the treatment of Guillain-Barré syndrome
Recovery from GBS
Guillain-Barré syndrome damages both nerve endings and other tissues in the body. The patient often needs comprehensive rehabilitation, which must resume physical activity and the necessary skills in everyday life. For this, massage, electrophoresis, relaxing baths, a contrast shower to raise muscle tone, physiotherapy, therapeutic exercises and much more are usually used. All this will give the patient the opportunity to return to a full life and no longer remember the syndrome.
Prevention of recurrence of the syndrome
There are no special techniques that can protect against GBS recurrence. But by following simple recommendations, you can at least make the risk of the disease less:
- refuse vaccination for at least six months;
- do not visit countries that have reported outbreaks of Zika virus or other dangerous infections;
- regularly visit neurologists and rehabilitation specialists at the clinic;
- temporary disability can be issued to reduce possible workloads.
Forecast for the future
Mortality in GBS is quite low - only up to 5%. It is caused by the most severe manifestations of the syndrome - weakening of breathing, immobilization and associated complications - pneumonia, pulmonary embolism and sepsis. The older the patient, the higher the chance of death.
Most people - about 85% - will fully recover and return to a fulfilling life. Moreover, only some of them will have the disease again, the rest will leave it in the past forever.
WHO about the syndrome
The World Health Organization is taking a number of measures to reduce the incidence and increase the number of people cured. She improves surveillance of epidemics of viral infections, in particular Zika, makes recommendations for therapy, supports GBS research programs around the world.
Guillain-Barré syndrome is a serious illness, but even if you have been diagnosed with it, you should not despair. Timely diagnosis and comprehensive treatment will quickly put you on your feet, literally and figuratively. Enjoy life, be healthy and take care of yourself.
Guillain-Barré syndrome is one of the most severe neurological diseases, which in every third patient at the height of the disease requires treatment in the intensive care unit. The term denotes a rapidly progressive neuropathy characterized by flaccid paralysis in symmetrical muscles of the limbs with sensory and autonomic disorders. The condition develops acutely, usually after suffering colds and other infections. However, with adequate treatment, full recovery is possible.
Causes
Guillain-Barré disease is commonly referred to as an autoimmune disease. Having coped with the infection, the human immune system does not recognize this and begins to attack its own body, in particular the nervous tissue. The cells of the immune system produce antibodies that lead to demyelination, that is, damage to the myelin sheath of the nerves. As a result of autoimmune processes, axons can also be damaged - processes involved in the innervation of muscles and internal organs.
The first signs of the disease are recorded one to three weeks after such infectious diseases as:

- Viral enteritis.
- Respiratory infections (ARVI).
- Cytomegalovirus infection.
- Infectious mononucleosis.
Signs of the development of the syndrome appear much less often after:
- Operations.
- Injury.
- With systemic lupus erythematosus.
- In HIV carriers.
- With malignant neoplasms.
Medical studies have not confirmed the connection between the occurrence of Guillain-Barré syndrome and influenza vaccination.
Kinds
Guillain-Barré syndrome is usually divided into two types - demyelinating and axonal; the first variant of peripheral nerve damage is more common.
- Demyelinating. Only the myelin sheaths are included in the pathological process, the destruction of axon cylinders is not detected. This leads to a slowdown in the speed of impulses, which provokes the development of reversible paralysis. Pathological changes affect the anterior, less often the posterior roots of the spinal cord; lesions of other parts of the central nervous system are also possible. The demyelinating type is considered a classic variant of the syndrome.
- In the axonal variant, the axial cylinders of the axons are also affected, which leads to the development of severe paresis and paralysis. The axonal type of polyneuropathy is considered more severe, after which motor functions are not fully restored.
Guillain-Barré syndrome occurs with self-limitation of the development of autoimmune processes. This means that sooner or later the immune cells stop their attack and the body begins to recover even in the absence of specific treatment.
However, in any case, the patient needs medical supervision and, possibly, an intensive course of supportive therapy - ventilation of the lungs, tube feeding, prevention of secondary infection, etc.
Symptoms
If, after an infection, a person does not feel recovered, but notices the following symptoms:
- subfebrile temperature;
- tingling and goose bumps in the fingertips;
- muscle pain of different localization;
- growing weakness
This is a reason to see a doctor immediately. The disease usually develops quickly and there is no time to waste.
The first symptoms of the disease include:

- Tetraparesis growing over several days - weakness in the lower and upper limbs. Tetraparesis is usually symmetrical, with flaccid tendon reflexes and low muscle tone on examination.
- In the first days, weakness is noted only in the legs - a sick person notices that it is more difficult for him to climb stairs.
- Chilliness of the limbs, as well as sweating, may disturb.
Sensory disturbances occur with a decrease or increase in sensitivity in the distal parts of the arms and legs. The pathological process can involve the muscles of the neck, respiratory muscles, less often the muscles of the eyes.
With severe damage, there is a violation of the function of swallowing and breathing, a patient with similar symptoms needs intensive care, up to tracheal intubation. The maximum development of all signs is observed in the third week of the disease. In some forms of the development of the disease, atypical symptoms are also detected:
- Increased blood pressure.
- Arrhythmias.
- Retention of urine.
- Paresis of the facial muscles.
Vegetative disturbances can lead to severe arrhythmias and cardiac arrest, which are often the leading cause of death.
The increase in symptoms is observed for two weeks, then the disease turns into a stabilization vase, lasting up to 4 weeks. The recovery phase lasts on average from one to two months, in some patients it is possible to achieve normalization of functions only after one to two years.
The disease can be suspected already upon questioning and examining the patient. For Guillain-Barré syndrome, symmetrical limb lesions and preservation of the function of the pelvic organs are characteristic. Of course, there are atypical signs of the disease, so a number of studies are necessary for differential diagnosis.

- Electromyography - determination of the speed of passage of an impulse along nerve fibers.
- A lumbar puncture can detect protein in the cerebrospinal fluid. Its content increases a week after the onset of the disease and reaches its peak by the end of the first month of the disease.
- EGC can detect arrhythmias.
- In blood tests, ESR and the number of leukocytes increase without other signs of infection.
In favor of confirming the diagnosis, the rate of increase in symptoms (no more than 4 weeks) and the recovery period lasting up to two months speaks. The disease must be differentiated from:
- Spinal cord tumor.
- Poliomyelitis.
- Botulism.
- Diphtheria polyneuropathy.
- Intoxication with salts of heavy metals.
In many cases, the outcome of the disease also depends on correct and early diagnosis.
Treatment
Treatment of Guillain-Barré syndrome is divided into two complementary types: non-specific and specific therapy. Treatment of patients with acute development of symptoms, impaired respiratory function, severe cardiac arrhythmias begins with non-specific therapy. The patient is admitted to the intensive care unit. In the phase of increasing symptoms, constant monitoring of respiratory function and cardiac activity is carried out.
Specific therapy includes the introduction of immunoglobulin and plasmapheresis.

- Immunoglobulin is given intravenously. This is especially necessary for those patients who cannot move without assistance, with difficulty swallowing and breathing.
- Plasmapheresis is prescribed for moderate to severe illness. Its use significantly accelerates the recovery time and prevents the development of residual phenomena. With a mild course of the disease, plasmapheresis is not used.
- With arrhythmias, increased blood pressure and other autonomic disorders, symptomatic therapy is used.
With paralysis, pressure sores and pneumonia are prevented, for which the patient is turned over, the body is treated, and massage is performed.
During the rehabilitation period, it is necessary to use complexes of physical exercises, physiotherapy, massage courses. In case of speech impairment, classes with a speech therapist are necessary.
Prevention
There is no specific prevention of the disease. Doctors can only recommend treating all infectious diseases at the very beginning of their development, this will reduce the negative effect of pathogens on the nervous system.
Patients with previous Guillain-Barré syndrome should refrain from any vaccinations for at least six months. Recurrence of the disease can occur after any other infectious disease, so it is necessary to avoid possible sites of infection.
Forecast
In almost 80% of cases, the lost functions are fully restored, in some patients minor movement disorders may be observed. In about 3% of cases, patients become disabled. Mortality is due to the lack of adequate therapy for the development of arrhythmias and heart failure, therefore, all patients with the syndrome should be under the supervision of health workers at the height of the disease.
Guillain-Barré syndrome is a disease in which the sheath of nerve fibers (myelin) is destroyed, which leads to impaired movement, sensitivity disorders. It usually develops some time after the infection.
Myelin is a special sheath of nerve fibers that is needed to conduct nerve impulses. In Guillain-Barré syndrome, it is destroyed by the body's own immune system. Normally, the immune system detects and destroys foreign objects (for example, pathogens of infectious diseases), but in some cases it begins to fight with native cells. As a result of damage to the myelin sheath, manifestations of the disease occur: decreased strength in the muscles, tingling in the extremities, etc. Most patients require hospitalization.
Timely started treatment allows you to achieve complete recovery, although some people may still have weakness in the muscles, a feeling of numbness.
Synonyms Russian
Acute inflammatory demyelinating polyradiculoneuropathy, acute polyradiculitis.
Synonymsenglish
Guillain-Barre syndrome, Acute Idiopathic Polyneuritis, Acute Inflammatory Demyelinating Polyradiculoneuropathy.
Symptoms
- Decreased strength in the muscles, tingling - first in the legs, then in the overlying parts of the body
- Intense pain in the shoulder girdle, back, hips
- Violation of chewing, swallowing, pronunciation of sounds, facial expressions as a result of a decrease in the strength of the muscles that perform these functions
- Increased or slowed heart rate
- Increase or decrease in blood pressure
- Respiratory disorders, with an increase in which artificial ventilation of the lungs may be required (carried out by a special apparatus when spontaneous breathing is ineffective)
- Retention of urine
- Constipation
General information about the disease
Guillain-Barré syndrome is a disease in which the myelin sheath of nerves is destroyed, as a result of which the conduction of nerve impulses is impaired and the strength in the muscles decreases.
The exact causes of the disease are unknown. In most cases, symptoms appear 1-3 weeks after an acute infection of the respiratory system, gastrointestinal infections.
These infections can be caused by these and other pathogens:
- campylobacter - found in the meat of infected birds and cause gastrointestinal infection when ingested with food;
- influenza virus;
- epstein-Barr virus (causative agent of infectious mononucleosis);
- mycoplasma - can cause pneumonia in people infected with the immunodeficiency virus (HIV).
Also, the triggering factor for the development of the disease can be vaccinations, surgical interventions.
Autoimmune mechanisms also play an important role. The immune system fights against foreign objects that enter the body. In response to infection, special protein particles are produced - antibodies. They detect and neutralize various infections and viruses. According to the researchers, in Guillain-Barré syndrome, antibodies not only destroy infectious agents, but also damage the membrane of nerve cells, this is possible due to the similarity in the molecular structure of these objects.
The myelin sheath covers nerve fibers and provides a certain speed of nerve impulses between the brain and various structures of the body. Violation of the passage of nerve impulses to muscle fibers leads to a decrease in strength in the muscles. The nerve fibers of the autonomic nervous system (which regulates the activity of internal organs) are also affected. In this case, the work of the cardiovascular system can be disrupted, the heart rhythm, blood pressure, etc.
In severe forms of the disease, the following complications are possible.
- Breathing disorder. It occurs as a result of weakness or paralysis (complete lack of ability to move) of the respiratory muscles and threatens the patient's life. In cases where spontaneous breathing is ineffective, artificial ventilation of the lungs is carried out (using a special apparatus).
- Disturbances in the work of the cardiovascular system.
- Prolonged immobility. Increases the risk of thromboembolism (blockage of blood vessels by blood clots, leading to poor circulation).
- Pressure ulcers are dead skin, underlying soft tissues that occur with prolonged immobility of patients due to a violation of blood supply.
The disease develops within a few weeks, and it may take several months to restore the lost functions. In most cases, complete recovery occurs.
Who is at risk?
- Persons of young and old age.
- Patients with certain types of infectious diseases.
- Underwent surgical interventions.
Diagnostics
Diagnosis of Guillain-Barré syndrome is quite difficult, since there are no specific studies to identify it. In this case, the diagnosis is based on the analysis of clinical manifestations, the study of the history of the disease, analyzes to exclude other diseases of the nervous system.
Laboratory diagnostics is of great importance.
- The protein is common in the cerebrospinal fluid. Cerebrospinal fluid (CSF) washes the brain and spinal cord. Various diseases of the nervous system cause certain changes in its composition. In Guillain-Barré syndrome, the level of protein in the cerebrospinal fluid increases.
To rule out other diseases, the following laboratory tests may be required:
- ... Allows you to determine the number of formed elements in the blood:,. A decrease in the number of erythrocytes and, possibly, with an increase in the level of leukocytes, with various inflammatory processes.
- ... This indicator deviates from the norm for various diseases, in particular, it increases with inflammatory processes in the body.
- ... With an insufficient amount of vitamin B 12 in the body, anemia and disturbances in the functioning of the nervous system may develop. Some of the symptoms of damage to the nervous system in B 12 deficiency anemia are similar to the manifestations of Guillain-Barré syndrome.
- Detection of heavy metals in urine. The accumulation of heavy metals (for example, lead) in the body contributes to damage to the nervous system and the development of polyneuropathy (damage to various nerves).
Other studies:
- Electromyography. Allows you to fix electrical impulses that travel along the nerves to the muscles. According to their intensity, the conductivity of nerve fibers is assessed; for this, special electrodes are applied to the muscle under study. The study is carried out in a calm state and with muscle contraction.
Additional research
- Magnetic resonance imaging (MRI). A diagnostic method based on the effect of a magnetic field on the human body. After processing the received signals, layer-by-layer images of the internal structures of the body are obtained. Allows to exclude the presence of other diseases of the nervous system (for example, masses).
Treatment
Treatment of the disease is conservative. Various drugs are used to eliminate individual manifestations of the disease, to combat the complications of Guillain-Barré syndrome.
The most effective are the following techniques:
- Plasmapheresis. Blood is taken from the patient, which is divided into a liquid part (plasma) and a part containing blood cells (erythrocytes, leukocytes, platelets). The blood cells are then returned to the human body, and the liquid portion is removed. This achieves a kind of purification of blood from antibodies that can destroy the myelin sheath of the nerves.
- Intravenous administration of immunoglobulin. Immunoglobulin contains antibodies from healthy blood donors. They block the destructive effect of the patient's antibodies on the nerve sheath.
It is very important to maintain the impaired functions of the body (artificial ventilation of the lungs), to carefully look after the patient, to prevent complications associated with prolonged immobility of patients.
In the recovery period, physiotherapy exercises, physiotherapy are used to restore the strength of various muscle groups.
Prevention
There is no specific prophylaxis for Guillain-Barré syndrome.
- Total protein in cerebrospinal fluid
Literature
- Dan L. Longo, Dennis L. Kasper, J. Larry Jameson, Anthony S. Fauci, Harrison's principles of internal medicine (18th ed.). New York: McGraw-Hill Medical Publishing Division, 2011. Chapter 385. Guillain-Barré Syndrome.
- Corey Foster, Neville F. Mistry, Parvin F. Peddi, Shivak Sharma, The Washington Manual of Medical Therapeuticts (33th ed.). Lippincott Williams & Wilkins Philadelphia, 2010.23 Neurologic Disorders. Guillain-Barré Syndrome.
RCHD (Republican Center for Healthcare Development of the Ministry of Health of the Republic of Kazakhstan)
Version: Clinical Protocols MH RK - 2016
Guillain-barré syndrome (G61.0)
Neurology
general information
Short description
Approved
Joint Commission on the Quality of Medical Services
Ministry of Health and Social Development of the Republic of Kazakhstan
dated November 29, 2016
Minutes No. 16
Guillain-Barré Syndrome (Guillain-Barrésyndrome) (GBS) is an acute, rapidly progressive autoimmune lesion of the peripheral nervous system, manifested in the form of paresthesia of the limbs, muscle weakness and / or flaccid paralysis (monophasic immune-mediated neuropathy). Synonyms for Guillain-Barré syndrome: acute inflammatory demyelinating polyneuropathy, acute idiopathic polyneuropathy, infectious polyneuropathy (polyneuropathy), acute polyradiculitis, Guillain-Barré-Strohl syndrome (Guillain-Barré-Barré-Strohlsyndrome) (Guillain-Barré-Strohlsyndrome) Landry-Guillain-Barré-Strohlsyndrome syndrome, Landry'ssyndrome syndrome, Landry's ascendingparalysis, French poliomyelitis (Frenchpolio), etc.
A feature of this disease is a self-limiting, monophasic course with extremely rare relapses. The ratio of the codes ICD-10 and ICD-9
|
CodeMKB-10
|
ICD-9 code
|
G61.0
|
Guillain-Barré Syndrome
|
357.0
|
Guillain-Barré Syndrome
|
|
|
|
|
|
Date of development / revision of the protocol:2016 year. Protocol users: GPs, therapists, resuscitators, neuropathologists (adults, children). Evidence level scale:
|
AND
|
High-quality meta-analysis, systematic review of RCTs, or large RCTs with very low likelihood (++) of bias whose results can be generalized to the relevant population.
|
|
AT
|
High quality (++) systematic review of cohort or case-control studies or High-quality (++) cohort or case-control studies with very low risk of bias or RCTs with low (+) risk of bias, the results of which can be generalized to the relevant population.
|
|
FROM
|
A cohort or case-control study or controlled study without randomization with a low risk of bias (+).
Results that can be generalized to the relevant population or RCTs with very low or low risk of bias (++ or +), the results of which cannot be directly extended to the relevant population.
|
|
D
|
Case series description or uncontrolled research or expert opinion.
|
Classification
Classification GBS refers to both the number of neuroinfections and post-infectious conditions. Several forms of GBS are distinguished, differing in the characteristics of the course of the pathological process, the primary point of application of autoimmune aggression (nerve sheath or axonal rod), recovery prognosis, and clinical manifestations. According to modern ideas, there are at least 8 varieties (clinical variants / subtypes) of Guillain-Barré syndrome:
1) acute inflammatory demyelinating polyneuropathy (the classic form of Guillain-Barré syndrome);
2) acute motor-sensory axonal neuropathy (OMSAN);
3) acute motor-axonal neuropathy (OMAN);
4) Miller-Fisher syndrome (SMF);
5) acute panautonomous neuropathy (acute panautonomous Guillain-Barré syndrome, acute pandizautonomy);
6) stem Bickerstaff encephalitis (Bickerstaff);
7) pharyngo-cervico-brachial variant;
8) acute cranial polyneuropathy.
There are also options for combining Miller-Fisher syndrome with other forms of Guillain-Barré syndrome (MFS / GBS overlapsyndrome). GBS is also classified according to the severity of the condition, depending on the clinical manifestations:
· Mild form is characterized by the absence or minimal paresis, which does not cause significant difficulties in walking and self-care;
With moderate severity, there is a violation of walking, limiting the patient in movement or requiring outside help or support;
With severe disease, the patient is bedridden and requires constant care, dysphagia is often observed;
In extremely severe form, patients require artificial lung ventilation (ALV) due to weakness of the respiratory muscles. Neurophysiological criteria for the classification of GBS (R.
Hadden,
D.
Cornblath,
R.
Hughesetal., 1998).
Group with primary demyelinating lesion:
the presence of at least one of the following signs in at least 2 nerves or two signs in one nerve is necessary if all other nerves are unexcited and the amplitude of the M-response at the distal point is 10% or more of the lower limit of the norm:
· The speed of propagation of excitation (SRV) is less than 90% of the lower limit of the norm, or less than 85% with the amplitude of the M-response at the distal point less than 50% of the lower limit of the norm;
· The distal latency of the M-response exceeds the upper limit of the norm by more than 10%, or more than 20% if the amplitude of the M-response at the distal point is lower than the lower limit of the norm;
· The presence of dispersion or block of excitation;
· F-wave latency exceeds the upper limit of the norm by more than 20%. Primary axonal lesion group:
There are no the above signs of demyelination in any nerve (excluding any one sign in 1 nerve, if the amplitude of the M-response at the distal point is more than 10% lower than the lower limit of the norm), and at least in two nerves the amplitude of the M-response at the distal point is more than 80% below the lower limit of the norm. Group with non-excitable nerves:
· M-response cannot be registered in any of the examined nerves or is present only in one nerve with an amplitude at the distal point more than 10% below the lower limit of the norm. Undefined group:
· The changes revealed during stimulation ENMG do not meet the criteria of any of the above groups.
Diagnostics (outpatient clinic)
DIAGNOSTICS AT THE AMBULATORY LEVEL Diagnostic criteria:
Complaints:
· Increasing muscle weakness in the arms and / or legs;
· Numbness and decreased sensitivity;
· Increased sensitivity (tactile, temperature, etc.) in the hands and feet;
· Pain in the back, shoulder and pelvic girdle;
· Violation of swallowing, both solid food and liquid;
· Violation of respiratory functions, up to the lack of spontaneous breathing, due to the weakening of the respiratory muscles, weakening of the voice and cough;
Heart rate disorder, in some it can be very frequent, in others it can be slowed down;
· Facial muscle paralysis;
· Increased sweating;
· Fluctuations in blood pressure;
· Possible occurrence of uncontrolled emission of urine;
• loss of tendon reflexes;
Shaky and unsure gait, impaired coordination of movements;
Changes in the volume of the abdomen, this happens because it is difficult for a person to breathe with the help of the diaphragm, and he is forced to use the abdominal cavity;
· Decreased visual acuity - most often there is a split and strabismus.
Symptoms are common in adults, children and newborns. Anamnesis:GBS develops, as a rule, 1-3 weeks after an infectious disease (ARVI, influenza, sinusitis, bronchitis, pneumonia, tonsillitis, measles, mumps, diarrhea, etc.).
Neurological symptoms appear suddenly; most patients have pain and paresthesias.
When taking a history, it is important to clarify the following aspects.
The presence of provoking factors. In approximately 80% of cases, the development of Guillain-Barré syndrome is preceded by one or another disease or condition in 1-3 weeks.
Infections of the gastrointestinal tract, upper respiratory tract, can develop after an intestinal infection caused by Campylobacterjejuni, after infections caused by herpes viruses (cytomegalovirus, Epstein-Barr virus, varicella-zoster virus), Haemophilusinfluenzae, mycoplasma, measles, mumps, Lyme and Lyme In addition, with HIV infection, the development of Guillain-Barré syndrome is possible.
· Vaccination (rabies, tetanus, influenza, etc.);
· Surgical interventions or injuries of any localization;
· Taking certain medicines (thrombolytic drugs, isotretinoin, etc.) or contact with toxic substances;
Sometimes Guillain-Barré syndrome develops against the background of autoimmune (systemic lupus erythematosus) and neoplastic (lymphogranulomatosis and other lymphomas) diseases. There is a certain pattern in the increase in symptoms, based on which 3 stages of the disease are distinguished:
· Progression (1-4 weeks) - the appearance and intensification of neurological disorders;
· Plateau (10-14 days) - stabilization of the clinical picture;
· Reverse development (from several weeks to 2 years) - restoration of the normal functioning of the body. Physical examinationincludes:
· general somatic status: general condition and its severity, body temperature, measurement of the patient's weight, examination of the skin, respiration, pulse, blood pressure, condition of internal organs (lungs, heart, liver, kidneys, etc.).
· neurological status:
Neurological examination is aimed at identifying and assessing the severity of the main symptoms of Guillain-Barré syndrome - sensory, motor and autonomic disorders.
· Assessment of the strength of the muscles of the limbs;
· Study of reflexes - areflexia is characteristic of Guillain-Barré syndrome (that is, the absence of most reflexes);
· Sensitivity assessment - the presence of areas of the skin with a feeling of numbness or tingling;
· Assessment of the function of the pelvic organs - possibly short-term urinary incontinence;
· Assessment of cerebellar function - the presence of unsteadiness in the Romberg position (standing with arms outstretched in front of you and closed eyes), lack of coordination of movements;
· Assessment of eyeball movements - with Guillain-Barré syndrome, there may be a complete lack of ability to move the eyes;
· Conducting vegetative tests - to assess damage to the nerves that innervate the heart;
· The reaction of the heart to a sharp rise from a lying position, physical activity is assessed;
· Assessment of the function of swallowing.
Assessment of the severity of motor deficit in children over 3 years old is carried out using the North American scale: Stage 0 Guillain Barré syndrome is the norm; Stage 1 - minimal movement disorders; Stage II - the ability to walk 5m without support or support; III stage - the ability to walk 5m with support or support; Stage IV - inability to walk 5m with support or support (confined to a bed or wheelchair); Stage V of Guillain-Barré syndrome - the need for mechanical ventilation; Stage VI - death. In clinical practice, to assess the severity of movement disorders, the scale of muscle strength of the limbs is used (A. Szobor, 1976). 0 points - there are no movements in the muscle. 1 point - minimal movements in the muscle, but the patient does not hold the weight of the limb. 2 points - the patient maintains the weight of the limb, but the resistance to the investigator is minimal. 3 points - the patient resists efforts to change the position of the limb, but it is insignificant. 4 points - the patient resists well the efforts to change the position of the limb, but there is some decrease in strength. 5 points - muscle strength corresponds to the age and constitutional norm of the subject.
Clinical options for ATP
|
Option
|
Main clinical symptoms
|
|
With a typical clinical picture
|
|
Acute inflammatory demyelinating polyradiculoneuropathy (typical GBS) (\u003e 85%)
|
Weakness in the limbs with relatively mild sensory impairments (possibly isolated movement disorders).
|
|
Acute motor axonal polyneuropathy (\u003e 5%)
|
Weakness in the limbs with no change in sensitivity. Deep reflexes can be saved. Fast restoration of functions. Mostly found in children.
|
|
Acute motor-sensory axonal polyneuropathy (\u003e 1%)
|
Weakness and sensory disturbances in the limbs. Rapid development of severe motor deficits with slow and incomplete recovery. Mostly found in adults.
|
|
With an atypical clinical picture
|
|
Miller-Fisher syndrome (\u003e 3%)
|
The combination of ataxia, mainly of the cerebellar type, with areflexia, ophthalmopolegy, sometimes mild weakness in the limbs. The sensitivity is usually preserved.
|
Laboratory research:
KLA - to exclude inflammatory diseases of internal organs, accompanied by polyneuropathic syndrome;
Blood sugar test (to exclude diabetic polyneuropathy);
· Biochemical blood tests - creatine, urea, AST, ALT, bilirubin (to exclude metabolic polyneuropathy);
Blood test for gas composition, electrolyte concentration - biochemical blood tests help to exclude metabolic polyneuropathies;
PCR of blood for hepatitis viruses - to exclude polyneuropathic syndrome in hepatitis
· Blood test for HIV infection - to exclude polyneuropathy associated with HIV infection;
· PCR blood test for viral infections (cytomegalovirus, Epstein-Barr virus, Borreliaburgdorferi, Campylobacterjejuni, etc.) - if an infectious etiology of GBS is suspected. Instrumental research:
· P-graphy of the chest organs - to exclude inflammatory lung disease or associated pulmonary complications with weakening of the respiratory muscles;
ECG - to identify or exclude vegetative heart rhythm disturbances in the GBS clinic;
· Ultrasound of the abdominal organs - diseases of the internal organs (liver, kidneys, etc.) can be accompanied by polyneuropathy similar to GBS;
· MRI of the brain * -necessary for differential diagnosis with the pathology of the central nervous system (acute cerebrovascular accident, encephalitis);
· MRI-spinal cord * - to exclude lesions (myelitis) at the level of the cervical thickening of the spinal cord (C4 - Th2);
Electroneuromyography ** (ENMG) - may be normal during the first week of the disease, with muscle damage, the denervation type of the ENMG curve is revealed, pulse conduction is slow, signs of damage to myelin or axons. Needle electromyography is characterized by the presence of signs of the current denervation-reinnervation process in polyneuropathy. Most often, the distal muscles of the upper and lower extremities are examined (for example, the anterior tibial muscle, the common extensor of the fingers), and, if necessary, the proximal muscles (for example, the quadriceps muscle of the thigh).
*NB!
Absolute contraindications to MRI are: a metal foreign body in the orbit; intracranial aneurysms clipped with ferromagnetic material; electronic devices in the body (pacemaker); hematopoietic anemia (for contrasting).
Relative contraindications for MRI are:
Severe claustrophobia;
· Metal prostheses, clips that are in non-scannable organs;
· Intracranial aneurysms, clipped with non-ferromagnetic material. **
NB!
ENMG is the only instrumental diagnostic method that allows to confirm lesions of the peripheral nervous system and the diagnosis of GBS, respectively, as well as to clarify the nature of pathological changes (demyelinating or axonal) and their prevalence. The protocol and scope of the ENMG study in patients with GBS depends on the clinical manifestations of the disease:
- with predominantly distal paresis, long nerves on the arms and legs are examined: at least 4 motor and 4 sensory (motor and sensory portions of the median and ulnar nerves; peroneal, tibial, superficial peroneal and sural nerves on one side). The main ENMG parameters are assessed:
· Motor responses (distal latency, amplitude, shape and duration), the presence of blocks of excitation conduction and dispersion of responses is assessed; the speed of propagation of excitation along motor fibers in the distal and proximal areas is analyzed;
· Sensory responses (amplitude) and the rate of conduction of excitation along sensory fibers in the distal regions;
· Late ENMG-phenomena (F-waves): latency, form and amplitude of responses, amount of chronodispersion, percentage of losses are analyzed.
- in the presence of proximal paresis, an additional study of two short nerves (axillary, musculocutaneous, femoral, etc.) with an assessment of the parameters of the motor response (latency, amplitude, shape) is mandatory.
It must be remembered that the first signs of a denervation process appear no earlier than 2-3 weeks after the onset of the disease, and signs of a reinnervation process - no earlier than 4-6 weeks. Diagnostic criteria for classical GBS by Asbury A. K. and Cornblath D. R.
based on clinical and laboratory data:
· The presence of progressive motor weakness with involvement of more than one limb in the pathological process;
Areflexia or severe hyporeflexia;
· CSF analysis - the presence of no more than 50 monocytes and / or 2 granulocytes 2+ in 1 μl of cerebrospinal fluid.
System for diagnosing GBS, the criteria of which are formulated by the National Institute for the Study of Neurological and Communication Disorders and Stroke (USA): Mandatory criteria:
· Progressive motor weakness in more than one limb; · The severity of paresis varies from minimal weakness in the legs to tetraplegia; · Suppression of reflexes of varying degrees. Auxiliary criteria for the diagnosis of the syndrome:
1.weakness increases within 4 weeks from the onset of the disease; 2. the relative symmetry of the lesion; 3. mild sensory impairment; 4. involvement of the cranial nerves in the pathological process; 5. recovery; 6. symptoms of autonomic dysfunction; 7. the usual absence of a febrile period at the onset of the disease; 8. an increase in the level of protein in the cerebrospinal fluid (CSF) 1 week after the onset of symptoms of the disease, provided that the number of mononuclear leukocytes usually does not exceed 10 cells in 1 mm3; 9. impairment of the conductive function of the nerves during the course of the disease in approximately 80% of cases; 10. absence of established causes of peripheral nerve damage, such as the effect of hexacarbon, porphyria, diphtheria, and other toxic and infectious diseases that mimic GBS.
Signs that absolutely exclude the diagnosis of GBS:
· Asymmetry of paresis;
• exclusively sensory disorders;
· Persistent pelvic disorders;
· Severe pelvic disorders;
· Recently transferred diphtheria;
· The presence of psychopathological symptoms - hallucinations, delirium;
· Proven poisoning with salts of heavy metals and others. Diagnostic algorithm:
Diagnostics (hospital)
DIAGNOSTICS AT STATIONARY LEVEL Diagnostic criteria at the inpatient level:see ambulatory level. Complaints and anamnesis:see ambulatory level. Physical examination:see ambulatory level. *
NB!
The criteria that are given in paragraph 9, subparagraph 1, are typical for GBS, axonal, paraparetic and pharyngo-cervico-brachial forms, and such forms as Miller Fisher syndrome and acute pandisautonomy clinically differ significantly from other forms of GBS, therefore, the generally accepted criteria for the diagnosis of this disease it is difficult to apply for them. The diagnosis in these cases is established primarily on the basis of anamnestic data and the clinical picture of the disease. Characteristics of Miller Fisher syndrome.
Stunning, confusion due to hyponatremia associated with overproduction of antidiuretic hormone. Convulsions may occur when plasma sodium levels are less than 120 mmol / L. Characteristics of acute pancreatic autonomy.
The emergence of neurological symptoms 1-2 weeks after the transferred viral or bacterial infection;
· The presence of an isolated lesion of the autonomic nervous system;
· Often the cardiovascular system is affected (postural hypotension, arterial hypertension, tachycardia, cardiac arrhythmias);
Blurred vision, dry eyes, anhidrosis;
• dysfunction of the gastrointestinal tract (paralyticileus);
· Difficulty urinating, acute urinary retention;
· Increased sweating, bluish color of the skin of the hands and feet, cold extremities;
Stunning, confusion due to hyponatremia associated with overproduction of antidiuretic hormone. Seizures may occur with plasma sodium levels less than 120 mmol / L;
· Recovery is gradual and often incomplete. To make a diagnosis of Guillain-Barré syndrome, it is necessary to clearly find out the history of the development of the disease, in conjunction with an assessment of the neurological status, to compare it with the criteria for diagnosing GBS (WHO; 1993). It is advisable to carry out a lumbar puncture with a study of cerebrospinal fluid, as well as to confirm the neural level of the lesion and to clarify the form of the disease according to the ENMG examination. Diagnostic algorithm:
GBS should primarily be differentiated from conditions that can lead to the development of acute peripheral tetraparesis. Differential-diagnostic search is greatly simplified when using a unique algorithm developed by researchers of the Federal State Budgetary Institution "NTSN" RAMS. Differential-diagnostic algorithm for acute flaccid tetraparesis (OBT) 
Note:OBT-acute flaccid tetraparesis; EMG electromyography; PNP polyneuropathy; GBS - Guillain-Barré syndrome; LP - lumbar puncture; BHAK - biochemical blood test; RF - rheumatic factor; CRP - C-reactive protein; CPK - creatinine phosphokinase; MRI - magnetic resonance imaging (at least 1 T); CT - computed tomography. Laboratory research:see ambulatory level (for those surveys that were listed additionally). List of basic laboratory tests:
Blood for immunoglobulins - when planning specific therapy with class G immunoglobulins, it is necessary to determine the Ig fractions in the blood, a low concentration of IgA is usually associated with its hereditary deficiency, in such cases there is a high risk of developing anaphylactic shock (therapy with immunoglobulin is contraindicated);
· Studies of cerebrospinal fluid (cytosis, protein concentration). When analyzing cerebrospinal fluid, the following three indicators are usually considered to be among the diagnostic criteria confirming GBS:
The presence of a high protein content,
An increase in the fraction of albumin,
· No concomitant increase in cytosis.
Additionally, the following diagnostic tests can be recommended to confirm the diagnosis and clarify the features of GBS in a particular case:
· Blood test for autoantibodies to gangliosides, with obligatory examination of GM1, GD1a, and also GQ1b if the patient has oculomotor disorders;
· Blood test for IgA antibodies to Campylobacter jejuni;
· Study of the content of biomarkers of heavy chains of neurofilament, tau protein and gliofibrillar acidic protein in blood serum. Instrumental research: see ambulatory level. In severe cases of the disease (rapid progression, bulbar disorders), daily monitoring of blood pressure, ECG, pulse oximetry and a study of the function of external respiration (spirometry, peak flowmetry), monitoring of the function of external respiration (determination of the vital capacity of the lungs (VC ) for the timely identification of indications for transferring the patient to mechanical ventilation.
Differential diagnosis
GBS must be differentiated from other diseases manifested by acute peripheral paresis, primarily from poliomyelitis (especially in young children) and other polyneuropathies (diphtheria, with porphyria). In addition, lesions of the spinal cord and brain stem (transverse myelitis, stroke in the vertebrobasilar system) and diseases with impaired neuromuscular transmission (myasthenia gravis, botulism) may have a similar clinical picture.
Diagnosis
|
Rationale for differential diagnosis
|
Surveys
|
Exclusion criteria
diagnosis
|
|
Poliomyelitis (especially in young children)
|
Acute peripheral paresis
|
ENMG;
· Needle EMG;
· Consultation of a therapist;
Consultation
infectious disease specialist.
|
· Epidemiological history;
• the presence of fever in the onset of the disease;
· Symptoms from the gastrointestinal tract;
· Asymmetry of the lesion;
· Lack of objective sensory disorders;
· High cytosis in cerebrospinal fluid;
· The diagnosis of poliomyelitis is confirmed by virological or serological research.
|
Other polyneuropathies
(inflammatory: chronic inflammatory polyneuropathy with an acute onset, Sjogren's disease, Churg-Strauss disease, cryoglobulinemic vasculitis;
Infectious: associated with HIV, Lyme disease;
Toxic: diphtheria, porphyria, medicinal, acute alcoholic, in case of poisoning with heavy metals
Dysmetabolic: polyneuropathy of critical conditions, with renal, liver failure,
acute hyperglycemic polyneuropathy)
|
Acute peripheral paresis
|
ENMG;
· Needle EMG;
· Consulting therapist;
· Cons. Infectionist;
Biochemical exudates of blood and urine
|
· Signs of the current denervation-reinnervation process;
Porphyria is favored by a combination of predominantly motor polyneuropathy with severe abdominal pain, intestinal paresis, arterial hypertension, tachycardia, severe mental changes (from depression to delirium), sleep disturbances, and epileptic seizures.
Porphyria has a discoloration of urine, which becomes reddish in the light, and then a rich reddish-brown color
|
Transverse myelitis Damage at the level of the cervical thickening of the spinal cord (C4 - Th2) post-infectious (M. pneumoniae, Schistosoma), post-vaccination, viral (enteroviruses, herpes), myelitis associated with HIV, with demyelinating diseases of the central nervous system, with systemic diseases (systemic red lupus, Sjogren's disease, acute necrotizing
vasculitis)
|
Acute peripheral paresis
|
· MRI of the spinal cord and brain;
ENMG;
· Cons. therapist;
· Cons.infectionist.
|
· Segmental border of disturbance of sensitivity;
· Persistent pelvic disorders;
· Lack of involvement of mimic and respiratory muscles with gross tetraparesis.
|
Acute spinal circulation disorder in the vertebrobasilar basin.
(thrombosis of the vessels of the spinal cord, vascular malformation, aneurysm, compression, trauma, neoplasm of the spinal cord)
|
Acute peripheral paresis
|
· MRI of the brain and spinal cord;
ENMG;
· Cons. therapist;
· Cons. neurosurgeon.
|
· Acute development (usually within a few minutes);
• in most cases, depression of consciousness (coma);
· Definitively the diagnosis is confirmed by MRI of the brain / spinal cord.
|
|
Myasthenia gravis
|
Acute peripheral paresis
|
· ENMG.
|
· Variability of symptoms;
· Lack of sensory disorders;
· Characteristic changes in tendon reflexes;
· The diagnosis is confirmed by EMG (detection of the decrement phenomenon);
· Positive pharmacological test with proserin.
|
|
Botulism
|
Acute peripheral paresis
|
ENMG;
· Cons.infectionist.
|
Relevant epidemiological data,
Descending type of paresis propagation,
Preservation in some cases of tendon reflexes,
Lack of sensory disorders,
No change in whetherquore. |
Treatment abroad
Undergo treatment in Korea, Israel, Germany, USA
Get advice on medical tourism
Treatment
Preparations (active ingredients) used in treatment
Treatment (outpatient clinic)
TREATMENT AT THE AMBULATORY LEVEL Treatment tactics:
Suspicion of Guillain-Barré syndrome, even with minimal severity of symptoms, is the basis for emergency hospitalization, and symptomatic treatment is carried out at the outpatient stage, and when a diagnosis is made, they are sent to a hospital, and the patient and his relatives must be warned of a possible rapid deterioration of the condition. Non-drugtreatment:no. Drug treatment:
Symptomatic therapy:
· With an increase in blood pressure, nifedipine, 10-20 mg under the tongue, can be prescribed;
· To reduce tachycardia, propranalol is used, at an initial dose of 20 mg 3 times a day; then the dose is gradually increased to 80-120 mg in 2-3 doses, under the control of blood pressure, heart rate, ECG;
With bradycardia - atropine, for adults: IV bolus under the control of ECG and blood pressure - 0.5-1 mg, if necessary, the administration is repeated after 3-5 minutes; the maximum dose is 0.04 mg / kg (3 mg). Children - 10 mcg / kg;
to reduce pain, analgesics, non-steroidal anti-inflammatory drugs are administered:
· Ketorolac, orally once at a dose of 10 mg or repeatedly, depending on the severity of the pain syndrome, 10 mg up to 4 times a day. The maximum daily dose should not exceed 40 mg, or no more than 60 mg is administered intramuscularly for 1 administration; usually 30 mg every 6 hours.
· Diclofenac, intramuscularly. A single dose is 75 mg, the maximum daily dose is 150 mg (with a break between injections for at least 30 minutes).
Ibuprofen, 1-2 tablets 3-4 times a day; if necessary, 1 tablet every 4 hours. Do not take more than 4 hours later. The maximum daily dose for adults should not exceed 1200 mg (no more than 6 tablets in 24 hours). Algorithm of actions in emergency situations:measures of symptomatic therapy. Other treatments:no.
· Consultation of an infectious disease specialist - determination or exclusion of an infectious disease (infectious mononucleosis, Lyme disease, HIV, etc.);
· Consultation of a therapist - establishment or exclusion of a therapeutic disease (inflammatory disease of internal organs: lungs, kidneys, liver, etc.);
· Consultation of an endocrinologist, nephrologist, rheumatologist - if necessary, to exclude somatic pathology.
Preventive actions:
· There is no specific prophylaxis of the disease, doctors may recommend treating all infectious diseases at the very beginning of their development, this will reduce the negative effect of pathogens on the nervous system. Patient monitoring:
· Assessment of the general condition of the patient with a description of the condition of the skin; the patient's weight;
· Hemodynamic indices: the number of respiratory movements, A / D, heart rate, pulse;
· Assessment of neurological status.
· Etiopathogenetic treatment at this stage is not carried out, and therefore there are no indicators.
Treatment (ambulance)
DIAGNOSTICS AND TREATMENT AT THE STAGE OF EMERGENCY EMERGENCY Diagnostic measures:
Often GBS has an acute course and is potentially life-threatening, because, starting from the legs, the lesion progresses, spreads to the bulbar and other cranial nerves, and therefore the following measures are necessary: Swallowing assessment - with bulbar paralysis, swallowing disorder, to prevent aspiration
· Nasogastric tube. Breath assessment- Perhaps the development of progressive respiratory failure, and not only of the obstructive type due to bulbar paralysis, but also with damage to the phrenic nerve (a paradoxical type of breathing is characteristic - when inhaling, the anterior abdominal wall sinks) and intercostal.
· Intubation of the trachea (for further transfer of the patient to mechanical ventilation). Assessment of the work of the heart:
· ECG -decrease and even inversion of the S-T segment, increase in the Q-T interval, cardiac arrest is possible.
During transportation, it is important to take care of maintaining airway patency, carefully monitor blood pressure and heart rate, tachycardia, orthostatic hypotension, arrhythmia, etc. Drug treatment:
· Syndromic therapy according to the protocol of emergency medical care.
Treatment (hospital)
STATIONARY TREATMENT Treatment tactics:The main goal of the treatment is: restoration of vital functions, elimination of symptoms of an autoimmune disease using specific techniques, the patient's rehabilitation period, prevention of complications. The first thing to do is to place the patient in a hospital, and, if necessary, connect him to a ventilator, install a catheter if urine is not emitted, install a nasogastric tube if swallowing is difficult. Non-drug treatment:
In severe cases with severe paresis, proper care is of particular importance for the prevention of complications associated with prolonged immobility of the patient (infection, pressure sores, pulmonary embolism). It is necessary to periodically (at least once every 2 hours) change the position of the patient, skin care, control over the functions of the bladder and intestines, passive gymnastics, and prevention of aspiration. With persistent bradycardia, the threat of asystole may require the installation of a temporary pacemaker. Drug treatment:
Specific therapy for Guillain-Barré syndrome, aimed at arresting the autoimmune process, is currently used pulse therapy with class G immunoglobulins and plasmapheresis (see paragraph - other types of treatment). The effectiveness of each of the methods is relatively the same, therefore, their simultaneous use is considered inappropriate.
Immunoglobulin G class, like plasmapheresis, reduces the duration of stay on mechanical ventilation; it is administered intravenously daily for 5 days at a dose of 0.4 g / kg. Possible side effects: nausea, head and muscle aches, fever.
Symptomatic therapy for Guillain-Barré syndrome is carried out to correct violations of acid-base and water-electrolyte balance, correct blood pressure, prevent deep vein thrombosis, thromboembolism.
Infusion therapy for the correction of violations of acid-base, water-electrolyte balances, severe arterial hypotension.
With persistent severe arterial hypertension, antihypertensive drugs are prescribed (β-blockers or blockers of slow calcium channels) (see KP Arterial hypertension).
With severe tachycardia, appoint (β-blockers (propranolol), with bradycardia - atropine (see below).
With the development of intercurrent infections, antibiotic therapy is required (drugs of a wide spectrum of action are used).
For the prevention of deep vein thrombosis and pulmonary embolism, low molecular weight heparin is prescribed in prophylactic doses twice a day).
For pain of nociceptive origin (muscle, mechanical) NSAIDs are recommended, in case of neuropathic pain, the drugs of choice are gabapentin, carbamazepine, pregabalin (only for adults!) (See below). List of essential medicines:.
|
Drugs
|
Single dose
|
Multiplicity of introduction
|
|
Immunoglobulin class G
|
0.4 g / kg i.v.
|
... 0.4 g / kg / day for 5 days 1 time per day, 5 days.
|
|
gabapentin
|
300 mg
|
1 day 300 mg 1 time / day, 2 day 300 mg 2 times / day, 3 day 300 mg 3 times / day, then,
depending on individual tolerance and effectiveness, the dose can be increased by 300 mg / day every 2-3 days to a maximum of 3600 mg / day.
|
|
carbamazepine
|
200 mg
|
The recommended starting dose is 200-400 mg per day. The dose can be gradually increased until a satisfactory clinical effect is obtained, in some cases it can be 1600 mg per day. After the pain syndrome goes into remission, the dosage can be gradually reduced.
|
|
pregabalin
|
150 mg
|
Treatment begins with a dose of 150 mg per day, divided into two or three doses. Depending on the patient's individual response and tolerance, after 3-7 days, the dose can be increased to 300 mg per day, and if necessary, after another 7 days, up to a maximum dose of 600 mg per day.
|
List of additional medicines:.
|
Drugs
|
Single dose
|
Multiplicity of introduction
|
|
nifedipine
|
10 mg
|
1-2 times under the tongue
|
|
Propranalol
|
10 mg
|
20 mg 3 times / day, then the dose is gradually increased to 80-120 mg in 2-3 doses, under the control of blood pressure, heart rate, ECG
|
|
Atropine
|
0,5-1,0
|
for adults: intravenous bolus under the control of ECG and blood pressure - 0.5-1 mg, if necessary, the administration is repeated after 3-5 minutes; the maximum dose is 0.04 mg / kg (3 mg). Children - 10 mcg / kg.;
|
|
Ketorolac
|
10 mg
|
inside once at a dose of 10 mg or repeatedly, depending on the severity of the pain syndrome, 10 mg up to 4 times a day. The maximum daily dose should not exceed 40 mg, or no more than 60 mg is administered intramuscularly for 1 administration; usually 30 mg every 6 hours. Not used in children.
|
|
Diclofenac
|
75 mg
|
intramuscularly, a single dose of 75 mg, the maximum daily dose is 150 mg (with an interval between injections of at least 30 minutes). Children are not applicable.
|
|
Ibuprofen
|
0.2 g
|
1-2 tablets 3-4 times a day; if necessary, 1 tablet every 4 hours. Do not take more than 4 hours later. The maximum daily dose for adults should not exceed 1200 mg (no more than 6 tablets in 24 hours).
Children: 10-20 mg / kg 3 times a day for 2-3 days.
|
Surgical intervention, indicating the indications for surgery: Surgical intervention may be required for tracheostomy in case of prolonged mechanical ventilation (more than 10 days), as well as gastrostomy in case of severe and prolonged bulbar disorders. Other treatments:
You should always remember the exceptional importance of a complex of rehabilitation measures for the prevention of complications due to immobility of the patient and for maintaining the functional state of the muscles until a sufficient volume of independent movements appears.
The patient needs:
- Physiotherapy
- Massage has a beneficial effect on the metabolism, which also accelerates the growth of nerves and reinnervation
- Physiotherapy to prevent the formation of contractures (electrical stimulation, heat therapy, drug electrophoresis, etc.).
- Hyperbaric oxygenation.
Membrane plasmapheresis significantly reduces the severity of paresis and the duration of mechanical ventilation. As a rule, 4-6 sessions are carried out with an interval of one day; the volume of plasma to be replaced in one session should be at least 40 ml / kg. A 0.9% sodium chloride solution or rheopolyglucin is used as replacement media.
It should be remembered about contraindications for plasmapheresis (infections, blood clotting disorders, liver failure), as well as possible complications (electrolyte disturbance, hemolysis, allergic reactions). Indications for specialist consultation:
· Consultation of an infectious disease specialist, if necessary (in the absence of a specialist at the prehospital level) - the establishment or exclusion of a chronic infection (brucellosis, borreliosis, etc.), as well as in case of confirmation of an infectious agent for the correction of etiological therapy;
· Consultation of a therapist, if necessary (in the absence of a specialist at the prehospital level) - establishment or exclusion of a therapeutic disease (inflammatory disease of internal organs: lungs, kidneys, liver, etc.), correction of hemodynamic parameters, electrolyte balance during therapy;
· Consultation with an ICU doctor - treatment of patients with severe forms of Guillain-Barré syndrome is carried out in conjunction with a doctor of the intensive care unit;
· Consultation of a cardiologist - in case of severe cardiovascular disorders (persistent severe arterial hypertension, arrhythmias). Indications for transfer to the intensive care unit and intensive care unit:
· Severe and extremely severe neurological disorders;
· Instability of hemodynamics;
· Respiratory dysfunction. Treatment effectiveness indicators:
· Stabilization of immunological status (quantitative and qualitative composition of IgG blood and cerebrospinal fluid);
· Regression of focal neurological symptoms. Further management.
After normalization of the patient's state of health, he must be registered with a neurologist. In addition, it will be necessary to undergo preventive examinations in order to identify the prerequisites for a relapse of the disease in the early stages. Dispensary observation in the polyclinic at the place of residence.
After the end of the acute period, complex rehabilitation measures are necessary, the plan of which is made up individually, depending on the severity of residual symptoms (exercise therapy, massage, while thermal procedures are contraindicated!).
Patients who have undergone GBS. you should be informed about the need to observe a protective regime for at least 6-12 months after the end of the disease. Physical overload, overheating, hypothermia, excessive insolation, alcohol intake are unacceptable. Also during this period, you should refrain from vaccination.
Medical rehabilitation
is carried out in accordance with the Standard for organizing the provision of medical rehabilitation to the population of the Republic of Kazakhstan, approved by order of the Minister of Health of the Republic of Kazakhstan dated December 27, 2013 No. 759.
Palliative care
Depending on the type and severity of complications following the disease, additional treatment may be required, such as:
· Immobilized patients are prescribed heparin subcutaneously at a dose of 5000 U every 12 hours and temporary compression of the calf muscles to prevent deep vein thrombosis;
· Massage has a beneficial effect on the metabolism, which also accelerates the growth of nerves and reinnervation;
· Kinesiotherapy has been proven to stimulate reinnervation and restore muscle volume;
· Physiotherapy to improve strength, to prevent the formation of contractures (electrical stimulation, heat therapy, drug electrophoresis);
· Rehabilitation to develop daily skills and use adaptive products that help in daily life;
The patient may require orthopedic devices or other supportive methods to improve movement;
· Psychotherapy;
Hospitalization
Indications for planned hospitalization: no. Indications for emergency hospitalization:
· Patients with GBS are subject to hospitalization in the intensive care unit.
Information
Sources and Literature
- Minutes of the meetings of the Joint Commission on the Quality of Medical Services of the Ministry of Healthcare of the Republic of Kazakhstan, 2016
- 1. Bykova OV, Boyko AN, Maslova OI Intravenous use of immunoglobulins in neurology (literature review and own observations) // Nevrol. zhurn. - 2000, 5.P. 32-39. 2. Gekht BM, Merkulova DM Practical aspects of the clinic and treatment of polyneuropathies // Nevrol. zhurn.-1997.-№ 2.-С.4-9. 3. Piradov M.A., Suponeva N.A. “Guillain-Barré Syndrome: Diagnosis and Treatment. Guide for Doctors "-2011. 4. Suponeva N.A., Piradov M.A. "Intravenous immunotherapy in neurology" -2013. 5. Sladky J. T. Guillain-Barre Syndrome in Children // J. Child Neurol. 2004. V. 19. P. 191-200. 6. Schmidt B., Toyka K. V., Kiefer R. et al. Inflammatory infiltrates in sural nerve biopsies in Guillain-Barre syndrome and chronic inflammatory demyelinating neuropathy // 1996. V. 19. P. 474–487. 7. Khalili-Shirazi A., Hughes R. A., Brostoff S. W. et al. T cell responses to myelin proteins in Guillain-Barre syndrome // J. Neurol. Sci. 1992. V. 111. P. 200-203. 8. Van Rhijn I., Bleumink-Pluym N. M., Van Putten J. P. et al. Campylobacter DNA is present in circulating myelomonocytic cells of healthy persons and in persons with Guillain-Barre syndrome // J. Infect. Dis. 2002. V. 185. P. 262-265. 9. Cooper J. C., Ben-Smith A., Savage C. O. et al. Unusual T cell receptor phenotype V gene usage of gamma delta T cells in a line derived from peripheral nerve of a patient with Guillain-Barre syndrome // J. Neurol. Neurosurg. Psychiatry. 2000. V. 69. P. 522-524. 10. Ilyas A. A., Chen Z. W., Cook S. D. et al. Immunoglobulin G subclass distribution of autoantibodies to gangliosides in patients with Guillain-Barre syndrome // Res. Commun. Pathol. Pharmacol. 2002. V. 109. P. 115-123. 11. Tsang R. S., Valdivieso-Garcia A. Pathogenesis of Guillain-Barre syndrome // Expert Rev. Anti Infect. Ther. 2003. V. 1. P. 597-608. 12. Kieseier B. C., Kiefer R., Gold R. et al. Advances in underswtanding and treatment of immune-mediated disorders of the peripheral nervous system // Muscle Nerve. 2004. V. 30. P. 131-156. 13. Adams D., Gibson J. D., Thomas P. K. et al. HLA antigens in Guillain-Barre syndrome // Lancet. 1977. No. 2. P. 504-505. 14. Koga M., Yuki N., Kashiwase K. et al. Guillain-Barre and Fisher's syndromes subsequent to Campylobacter jejuni enteritis are associated with HLA-54 and Cwl independent of anti-ganglioside antibodies // J. Neuroimmunol. 1998. V. 88. P. 62-66. 15. Magira E. E., Papaijakim M., Nachamkin I. et al. Differential distribution of HLA-DQ beta / DR beta epitopes in the two forms of Guillain-Barre syndrome, acute motor axonal neuropathy and acute inflammatory demyelinating polyneuropatrhy (AIDP); identification of DQ beta epitopes associated with susceptibility to and protection from AIDP // J. Immunol. 2003. V. 170. P. 3074-3080. 16. Geleijns K., Schreuder G. M., Jacobs B. C. et al. HLA class II alleles are not a general susceptibility factor in Guillain-Barre syndrome // Neurology. 2005. V. 64. P. 44-49. 17. Asbury A. K., Cornblath D. R. Assessment of current diagnostic criteria for Guillain-Barre syndrome // Ann. Neurol. 1990. V. 27. S. 21-24.
Information
ABBREVIATIONS USED IN THE PROTOCOL
|
Cvdp
|
chronic inflammatory demyelinating polyradiculoneuropathy
|
|
Tnp
|
polyneuropathy
|
|
NMSP
|
hereditary motor-sensory polyneuropathy
|
|
GBS
|
guillain-Barré syndrome
|
|
HELL
|
arterial hypertension
|
|
PNS
|
peripheral nervous system
|
|
CNS
|
central nervous system
|
|
MRI
|
magnetic resonance imaging
|
|
PCR
|
polymerase chain reaction
|
|
CSF
|
cerebrospinal fluid
|
|
ESR
|
erythrocyte sedimentation rate
|
|
Ig
|
immunoglobulin
|
|
Heart rate
|
heart rate
|
|
AIDS
|
acquired immunodeficiency syndrome
|
|
EMG
|
electromyography
|
|
ENMG
|
electroneuromyography
|
|
IVIG
|
normal human immunoglobulin for intravenous administration
|
|
GK
|
glucocorticoids
|
List of protocol developers with qualification data:
1. Kayshibaeva Gulnaz Smagulovna, Candidate of Medical Sciences, JSC "Kazakh Medical University of Continuing Education", Head of the Department of Neurology, certificate "adult neuropathologist".
2. Zhumagulova Kulparam Gabibulovna, candidate of medical sciences, certificate "neuropathologist adult of the highest category", JSC "Kazakh Medical University of Continuing Education", Associate Professor of the Department of Neurology.
3. Tuleutaeva Raikhan Esenzhanovna, clinical pharmacologist, candidate of medical sciences, professor of RAE, head of the department of pharmacology and evidence-based medicine, Semey State Medical University. No Conflict of Interest Statement:no. List of reviewers:
Dushanova G.A. - Doctor of Medical Sciences, Professor, Head of the Department of Neurology, Psychiatry and Psychology of the South Kazakhstan State Pharmaceutical Academy. Indication of the conditions for revision of the protocol: Revision of the protocol 3 years after its publication and from the date of entry into force or when new methods with a level of evidence are available.
Attached files
Attention!
- Self-medication can cause irreparable harm to your health.
- The information posted on the MedElement website and in the mobile applications "MedElement", "Lekar Pro", "Dariger Pro", "Diseases: Therapist's Guide" cannot and should not replace an in-person consultation with a doctor. Be sure to contact a healthcare provider if you have any illness or symptoms that bother you.
- The choice of medicines and their dosage should be discussed with a specialist. Only a doctor can prescribe the necessary medicine and its dosage, taking into account the disease and the condition of the patient's body.
- MedElement website and mobile applications "MedElement", "Lekar Pro", "Dariger Pro", "Diseases: Therapist's Guide" are exclusively information and reference resources. The information posted on this site should not be used to unauthorized changes in the doctor's prescription.
- The MedElement editors are not responsible for any damage to health or material damage resulting from the use of this site.
Guillain-Barré syndrome is a severe autoimmune disease that affects the peripheral nervous system.
The most common manifestation is acute tetraparesis, when movement of all four limbs becomes almost impossible. Other movements also cease, including swallowing, the ability to lift the eyelids, and spontaneous breathing. Despite this, the course of the disease is benign, most cases end in recovery. Transition to a chronic course or relapses are less common.
Guillain-Barré syndrome occurs in all countries, regardless of their level of development, with the same frequency - about 2 cases per 100 thousand population, there is no sex dependence. The disease can affect patients of all ages.
What it is?
Guillain-Barré syndrome is an acute form of progressive inflammatory polyneuropathy characterized by muscle weakness and polyneuritic sensory disorder. The disease is also called acute idiopathic polyneuritis, Landry's palsy or inflammatory demyelinating polyradiculoneuropathy. The disease is a representative of autoimmune abnormalities.
Usually, the pathology has specific signs that make it possible to recognize it at the earliest stages of development and start adequate treatment on time. It has been proven that more than 80% of patients have a favorable prognosis and are completely cured.
Classification
There are several forms of Guillain-Barré syndrome, depending on the symptoms and the area of \u200b\u200bthe lesion:
- classical (80% of cases) - inflammatory demyelinating polyradiculoneuropathy;
- axonal (15%) - motor or motor-sensory neuropathy, which is accompanied by damage to the axons of nerve fibers responsible for the movement and sensitivity of muscles;
- miller-Fisher syndrome (3%) - a combination of ophthalmoplegia, areflexia with mild paresis and cerebellar ataxia;
- atypical (rare) - sensory neuropathy, pandizautonomy and cranial polyneuropathy.
Depending on the duration of the increase in the symptoms of the disease:
- acute - 7-14 days;
- subacute - 15-28 days;
- chronic - observed over a long period (up to several months), characterized by a slow development of symptoms and a change in periods of remission and deterioration.
Chronic Guillain-Barré disease is considered one of the most dangerous because it is difficult to diagnose, which significantly reduces the chances of starting timely treatment.
Etiology
In most cases, the reasons for the expression of Guillain-Barré syndrome are unclear, since it refers to an autoimmune process. But experts identify several predisposing factors:
- complex course of infectious diseases;
- damage to the upper respiratory tract;
- mononucleosis of an infectious nature;
- complications from surgery or vaccination;
- HIV infection;
- traumatic brain disease or trauma resulting in swelling or neoplasms in the brain. That is why the likelihood of the effect of the syndrome on the human nervous system is high;
- genetic predisposition. If a close relative has been diagnosed with this disease, then the person automatically falls into the risk zone. For this reason, the disease can manifest itself in a newborn child and school-age children;
- infections included in the group of herpes viruses.
Experts agree that Guillain-Barré syndrome is expressed during or after the course of the above diseases.

Symptoms
Guillain-Barré syndrome is characterized by certain symptoms, namely, relatively symmetrical muscle weakness (flaccid paresis), which typically begins in the proximal muscles of the legs and spreads to the arms after a few hours or days. Weakness is often accompanied by paresthesias of the toes and hands. Sometimes weakness primarily occurs in the arms or in the arms and legs at the same time.
The protein content in the cerebrospinal fluid rises (starting from the 2nd week of the disease). In severe cases, paralysis of the respiratory and cranial muscles occurs, mainly of the facial and bulbar muscles. Frequent pain in the back, shoulder and pelvic girdle, sometimes radiating along the roots, symptoms of tension. Patients, especially those with concomitant diabetes mellitus, are prone to the development of pressure ulcers.
In Guillain-Barré syndrome, pronounced autonomic disorders are often noted: an increase or decrease in blood pressure, orthostatic hypotension, sinus tachycardia, bradyarrhythmia, and transient urinary retention. Intubation or suction of mucus can cause severe bradycardia, collapse, and even cardiac arrest. Having reached a peak, the symptoms stabilize (the plateau phase lasts 2-4 weeks), and then recovery begins, which can last from several weeks to 1-2 years.
Death is possible from respiratory failure associated with paralysis of the respiratory and / or bulbar centers, pneumonia, thromboembolism of the pulmonary arteries, cardiac arrest, sepsis, but thanks to modern methods of intensive therapy, primarily mechanical ventilation, mortality in the last decade has decreased to 5%.
What is the danger?
Usually, the anomaly develops slowly over 2-3 weeks. First, there is a slight weakness in the joints, which intensifies over time and really begins to cause discomfort to the patient.
Immediately after the tingling sensation, in the acute course of the disease, there is general malaise, weakness in the shoulder and hip regions. Difficulty breathing appears after a few hours. In this case, it is imperative to seek help from the hospital. Usually, the patient is immediately connected to the artificial respiration system, and then the necessary medication and physiotherapy are provided.
In the acute form of the disease, pathology on the second or third day can completely paralyze any limb. Also, in the absence of timely treatment, the patient faces:
- Decreased immunity;
- Respiratory failure;
- Sedentary joints;
- Peripheral paralysis;
- Adaptation problems in society;
- Difficulty in life;
- Disability;
- Fatal outcome.
Diagnostics of the Guillain-Barré syndrome
Instrumental diagnostics
Lumbar puncture
With lumbar puncture, CSF results usually show elevated protein levels (\u003e 45 mg / dL), without pleocytosis (<10 клеток/мм3) (белково-клеточная диссоциация). Иногда уровень белка может оставаться нормальным, при умеренном повышении количества клеток (10-50 клеток/мм3). Цитоз выше, чем 50 клеток/мм3, свидетельствует против диагноза ГБС. В ряде случаев могут быть необходимы повторные люмбальные пункции для уточнения диагноза.
Neurofunctional diagnostics
ENMG (Electroneuromyography) is the only instrumental diagnostic method that allows you to confirm the diagnosis of GBS and clarify the nature of pathological changes (demyelinating or axonal) and their prevalence.
Needle electromyography is characterized by the presence of signs of the current denervation-reinnervation process in polyneuropathy. Examine the distal muscles of the upper and lower extremities (for example, the tibialis anterior muscle, the common extensor of the fingers), and, if necessary, the proximal muscles (for example, the quadriceps muscle of the thigh).
The ENMG study in patients with GBS depends on the clinical manifestations:
- with distal paresis, long nerves on the arms and legs are examined: at least four motor and four sensory (motor and sensory portions of the median and ulnar nerves; peroneal, tibial, superficial peroneal and sural nerves on one side).
Assessment of the main ENMG parameters:
- motor responses (distal latency, amplitude, shape and duration), the presence of blocks of conduction and dispersion of responses; the speed of propagation of excitation along motor fibers in the distal and proximal areas is analyzed.
- sensory responses: the amplitude and speed of excitation conduction along sensory fibers in the distal regions.
- late ENMG-phenomena (F-waves): latency, form and amplitude of responses, amount of chronodispersion, percentage of loss are analyzed.
- in case of proximal paresis, a study of two short nerves (axillary, musculocutaneous, femoral, etc.) with an assessment of the parameters of the motor response (latency, amplitude, shape) is mandatory.
The first signs of a denervation process appear two to three weeks after the onset of the disease, signs of a reinnervation process - after a month.
Treatment
Treatment of Guillain-Barré syndrome is carried out in a hospital setting. The patient needs proper care, hardware observation, drug therapy, and in some cases - urgent surgery.
Drug therapy is aimed at stopping the autoimmune reaction. The patient is shown class G immunoglobulins, which are administered intravenously. They have side effects such as nausea, fever and headache, but they improve respiratory function. Also, membrane plasmapheresis is performed, in which the patient's blood plasma is replaced with a chloride solution or preopolinlucinol. This reduces the severity of paresis and allows you to shorten the time to support the patient on the ventilator.
From the symptomatic treatment of Guillain-Barré syndrome, B vitamins, antihistamines, antipyretic and pain relievers, heart rate and pressure regulators, antithrombotic and anticholinesterase agents, and artificial tears are prescribed.
With prolonged bulbar disorders and the development of respiratory failure, tracheo- or gastrostomy is possible. Weakness and paralysis of the respiratory and bulbar muscles require monitoring of respiratory activity, heart rate, and blood pressure. Sometimes it is necessary to install a pacemaker, with a decrease in lung capacity by 25-30%, the use of a ventilator is indicated. Bulbar paralysis requires a nasogastric tube. You may also need to insert a catheter into your bladder.
Patient care includes the prevention of complications associated with immobility (bedsores, thrombosis, etc.). For this purpose, the position of the patient's body is changed every 2 hours. Cleansing of the skin, passive gymnastics, control over the work of the intestines and bladder are prescribed.
Rehabilitation
Rehabilitation of a patient with Guillain Barré syndrome is an integral part of any course of treatment, because a person needs to learn to serve himself: hold a spoon, dress, walk. For successful restoration of activity, doctors prescribe courses of massage, rubbing, hirudotherapy, therapeutic baths, wax applications, procedures with ozokerite. Patients are also advised to take physical therapy classes and follow a diet.

Prevention
There is no specific prevention of the disease. Doctors can only recommend treating all infectious diseases at the very beginning of their development, this will reduce the negative effect of pathogens on the nervous system.
Patients with previous Guillain-Barré syndrome should refrain from any vaccinations for at least six months. Recurrence of the disease can occur after any other infectious disease, so it is necessary to avoid possible sites of infection.
Forecast for life
Most often, with Guillain-Barré syndrome, the prognosis is favorable. Usually, normal functioning of the limbs is restored after 7-12 months in 85% of people. The disease becomes chronic in 7-15% of cases. The lethal outcome is approximately 5%. Respiratory failure, pneumonia, or viral infections can cause death. But most often all this can be prevented by contacting a specialist in time.
|





