Sections of the site
Editor's Choice:
- Heart transplant: the possibilities of modern surgery
- Types and reasons for taking a Coombs test
- Endocrine system Neurohypophysis histology
- Offset m echo what. Echoencephalography. For what diseases do echoencephalography
- Nephrotoxic effect of X-ray contrast agents
- Clinical anatomy of the anterior mediastinum Mediastinum: boundaries, division into departments
- Tinnitus causes, diagnosis and treatment
- Baralgin injection: instructions for use Baralgin injections instructions for use reviews
- What a stunned person feels
- Sympathetic and parasympathetic nervous system
Advertising
| Determination of the length and diameter of the spleen. Percussion and palpation of the spleen, diagnostic value. Spleen tapping according to M.G. Kurlov |
|
Can be carried out: either standing with arms raised up, or lying on the right side. First, the upper and lower borders of the spleen are determined. For this, the finger-plessimeter is installed in the transverse direction on the left lateral surface of the chest at the level of the V rib. The middle phalanx of the finger should lie on the mid-axillary line and be perpendicular to it. Percussion is conducted from top to bottom until the transition of a clear pulmonary sound to a dull one and mark on the side of a clear sound. Normally, the upper border of splenic dullness is located on the IX rib. To determine the lower border of splenic dullness, the finger-pessimeter is placed below the XII ribs and percussed along the same line in the direction from bottom to top until a dull sound appears. Normally, the lower border is at the level of the XI rib. The distance between the obtained points characterizes the width of the splenic dullness and is on average 4 cm. Determination of the anterior and posterior border of splenic dullness is carried out using percussion along the X edge. The finger-plessimeter is placed at the edge of the left costal arch perpendicular to this rib and percussed until the tympanic sound becomes dull. Normally, the anterior border of splenic dullness should not go beyond the left articular line (the line connecting the edge of the XI rib with the junction of the left clavicle with the sternum). To find the posterior border of splenic dullness, a finger-pessimeter is placed perpendicular to the X rib between the left posterior axillary and scapular lines and percussed along this rib anteriorly until a dull sound appears. By measuring the distance between these points, the length of the spleen is obtained (on average 6 cm). Percussion of the abdomen It is carried out downward from the navel in the supine and standing position and to the lateral surfaces in both directions. In the supine position, the pessimeter finger is placed longitudinally along the anterior midline so that its middle phalanx lies on the navel. Percussion along the umbilical line alternately in the direction of the right and left lateral parts of the abdomen until the transition of the tympanic sound to dull. Normally, on both sides, the border of the transition of the tympanic sound to the blunt one runs along the anterior axillary lines. A more medial location of the border indicates the accumulation of free fluid in the abdominal cavity. When the patient moves to an upright position, the fluid will move to the lower part of the abdominal cavity. Therefore, tympanitis will be determined in the lateral areas of the abdomen, and percussion along the vertical lines in the direction from top to bottom in the lower abdomen reveals an area of \u200b\u200bdull sound with a horizontal upper border. The spleen is an unpaired organ located on the left side of the abdominal cavity. The front of the organ is adjacent to the stomach, and the back to the kidney, adrenal gland and intestines. The structure of the spleenIn the composition of the spleen, the serous cover and its own capsule are determined, the latter formed by a combination of connective tissue, muscle and elastic fibers. The capsule passes into the skeleton of the organ, dividing the pulp (parenchyma) into separate "islets" with the help of trabeculae. In the pulp (on the walls of arterioles) there are round or oval nodules of lymphoid tissue (lymphoid follicles). The pulp is based on reticular tissue, which is filled with a variety of cells: erythrocytes (mostly decaying), leukocytes and lymphocytes. Organ functions
That is, the organ performs many important functions, and therefore, to determine the pathologies at the initial stages of the examination, it is first of all necessary to perform palpation and percussion of the spleen.
The sequence of palpation of internal organsAfter collecting complaints, anamnesis and a general examination, the doctor, as a rule, proceeds to physical research methods, which include palpation and percussion.
In case of suspicion of the presence of spleen diseases (or its enlargement due to liver diseases), percussion, palpation of the liver and spleen are mandatory.
General rules for palpationFeeling (palpation) of the spleen is one of the most informative physical research methods carried out by a doctor. In the case of a slight increase in the organ, when the spleen is not easy to palpate, the doctor necessarily recommends an ultrasound scan to confirm / refute the alleged pathology in a child or adult.
Spleen palpation: algorithm
Interpretation of resultsUnder normal conditions (in healthy people), the spleen is not palpable. The exception is asthenics (usually women). In other cases, it is possible to feel the spleen when the diaphragm is lowered (pneumothorax, pleurisy) and splenomegaly, that is, an increase in the size of the organ. A similar condition is more often observed in the following conditions:
Most often, palpation of even an enlarged spleen is painless. The exceptions are organ infarctions, rapid expansion of the capsule, perisplenitis. In these cases, the spleen becomes extremely sensitive (that is, painful on palpation). With cirrhosis of the liver and other chronic pathologies, the edge of the spleen is dense, while in acute processes it is soft. The consistency is usually soft in acute infections, in chronic infections and cirrhosis of the liver it becomes firm.
According to the degree of enlargement of the organ, the palpable part can be smaller or larger, and how far the spleen has come out from under the ribs may indicate the true degree of enlargement of the organ. So, a relatively small increase is indicated by the exit of the edge of the organ from under the costal arch by 2-7 centimeters, which is observed in acute infections (typhoid, meningitis, sepsis, lobar pneumonia, and so on) or chronic pathologies (heart disease, cirrhosis, erythremia, leukemia, anemia) and unexplained etiology, which often occurs in young people (possibly with hereditary syphilis, rickets) According to the density of the palpable edge of the spleen (with its increase), it is possible to draw conclusions about the age of the process. That is, the longer there is inflammation in the organ, the denser and harder its parenchyma, from which it follows that in acute processes the edge of the spleen is softer and more elastic than in chronic ones. If the organ is too large, when the lower edge is defined in the pelvic cavity, it is very easy to palpate the spleen, and no special skills are required. In the case of splenomegaly as a result of a neoplasm, palpation of the spleen (more precisely, its margo crenatus) determines notches (from 1 to 4). A similar diagnostic sign indicates the presence of amyloidosis, leukemia (myelogenous chronic or pseudo-leukemia), malaria, cysts and endotheliomas. That is, when palpating the spleen, the doctor has the opportunity to assess the condition of its surface, detect fibrin deposition (as, for example, with perisplenitis), various protrusions (which happens, for example, with abscesses, hemorrhagic and serous cysts, echinococcosis) and determine tissue density. With abscesses, swelling is often found. All the information determined by palpation is extremely valuable both for diagnosing a disease of the spleen itself, and for determining diseases that could lead to splenomegaly. Normally, the spleen is located in the region of the left hypochondrium, its long axis is located along the tenth rib. The organ has an oval (bean-shaped) shape.
Spleen in childhoodThe size of the spleen is normal depending on age:
It should be remembered that palpation of the spleen in children, as well as in adults, should be painless, in addition, normally the spleen in a child is not detected. The dimensions described above are not absolute, that is, small deviations in the direction of decreasing / increasing the size of the organ should not be regarded as a pathology.
Spleen percussionThis method is used to assess the size (boundaries) of an organ. The patient is placed in the right semi-lateral position with the arms above the head, while the legs are barely bent at the hip and knee joints. Percussion should be, moving from clear to dull sound, applying quiet percussion beats. The spleen is an unpaired parenchymal organ with an ovoid shape and a pointed lower pole. Located in the very depths of the left hypochondrium, with the anterior portion of its gastric (visceral) surface, it is adjacent to the stomach, and with the posterior lower portion (renal surface) - to the adrenal gland and kidney. From below, the organ of interest to us is in contact with the bend of the colon. Located under the left dome of the diaphragm (between the ninth and eleventh ribs), the spleen is endowed with respiratory mobility. Its long axis (the so-called "longitudinal") coincides normally with the course of the tenth rib. In people with an asthenic physique, the spleen is located slightly lower and more vertically, in those with a hypersthenic physique - higher and horizontally. Inspection tasksPalpation of the spleen pursues several tasks at once. With its help you can:
Before proceeding with palpation, a qualified doctor will certainly collect data to compile an anamnesis (history) of the disease. In most cases, this helps to establish the true cause of the disorders that prevent the normal functioning of the spleen. Visual inspectionThe first step in examining the spleen is an external examination of the abdomen, including:
In a healthy person, the appearance of the abdomen (its shape and size) always corresponds to gender, body type, level of physical development and degree of fatness. The presence of pathological processes in the spleen inevitably provokes its increase, which can be both insignificant and colossal (in the most severe cases, the organ can reach the level of the iliac fossa). Excessive enlargement of the spleen contributes to an increase in the size of the abdomen, in which it becomes asymmetric (due to the obvious bulging of the left half). In a patient who has taken a horizontal position, the outline of a pathologically enlarged spleen can be seen through the abdominal wall. To a greater extent, this is typical for extremely malnourished patients suffering from cachexia. The enlargement of the abdomen is accompanied by the smoothing or disappearance of the depression, which every healthy person has from the left edge of the costal arch. In some patients, even the lower part of the chest (on the left side) may protrude. PercussionEvery specialist performing percussion (tapping) of the spleen knows about the small size of this organ, located in the left hypochondrium so deeply that only two-thirds of its diaphragmatic surface located under the chest wall can be subjected to this manipulation. Since the area of \u200b\u200bthe spleen accessible for tapping is surrounded by organs containing air (lungs, intestines, stomach), the best option for studying it is direct quiet percussion according to Yanovsky, which results in absolute dullness. In the case of performing mediocre deep percussion (this option is quite possible), the specialist will determine only dullness due to the involvement of air-containing tissues in the percussion zone, which give voiced tympanic sounds when tapped. Using quiet percussion, you can determine the approximate size of the spleen. During the manipulation, the patient may:
It is in these positions of the subject's body that the liquid gastric contents are displaced to the right or downward from the spleen, significantly improving the conditions and results of palpation. To determine the upper border of the organ, a finger, playing the role of a pessimeter, is installed at the intersection of the mid-axillary line and the level of the sixth-seventh intercostal space and percussion is started, moving down the intercostal space. The signal to stop movement is the moment when a loud pulmonary sound gives way to a dull one. The border (with the help of a dermograph or by fixing the left hand with the little finger) is marked from the side of the tympanic sound. To establish the inferior border of the spleen, the pessimeter finger must be positioned on the mid-axillary line in a direction parallel to the expected border (just below the costal arch). The direction of percussion is carried out from bottom to top: from a clear sound to the beginning of dullness. The boundary is marked on the clear sound side. Determining the front border of the organ of interest to us, the finger-pessimeter is placed on the front wall of the abdomen (to the left of the navel, at the level of the tenth intercostal space) parallel to the proposed border. Percussion should be advancing to the transverse axis of splenic dullness until the first signs of dullness appear. The boundary mark is placed on the side where the clear sound comes from. The anterior border of the spleen should normally be one to two centimeters from the anterior axillary line (to the left of it). To identify the posterior border of the organ, the finger-pessimeter is installed perpendicular to the tenth rib (the direction of percussion should be parallel to the sought-for border). Moving between two lines (posterior axillary and scapular), percussion is performed until a slightly dull sound appears (from back to front). Having established the upper and lower boundaries of the investigated organ, measure the distance between them, resulting in the length of its diameter, located between the ninth and eleventh ribs. A length of four to six centimeters is considered normal. By measuring the distance separating the anterior and posterior border of the spleen, the value of its length is obtained (in healthy people it ranges from six to eight centimeters). The increased values \u200b\u200bof the transverse and long axis of the splenic dullness are indisputable evidence of an increase in this organ that occurs in patients suffering from:
In the presence of acute infectious diseases (especially with sepsis), the spleen acquires a soft consistency. A pronounced compaction of the organ is observed in cases of amyloidosis, with chronic infectious processes, blood diseases, oncological lesions, portal hypertension. Due to cysts, heart attacks, syphilitic gums, echinococcosis, the surface of the spleen becomes uneven. Soreness of the organ occurs as a result of its infarction, inflammation, as well as splenic vein thrombosis. How spleen percussion is performed is described in this video:
Norms in children and adultsIn the protocol of ultrasound examination of the spleen, the specific values \u200b\u200bof its three linear dimensions must be indicated (information that the organ is enlarged, not supported by numbers, is an answer). The normal size of the spleen (on average) in adult patients is presented in the list below:
The mass of a healthy spleen in women does not exceed 150 g, in men it ranges from 190 to 200 g. Another indicator of the normal state of the organ of interest to us is the area of \u200b\u200bthe maximum cut. Its normal value is between forty and fifty square centimeters. It must be understood that the above values \u200b\u200bare averaged, since the size of any internal organs is individual for each person. The parameters of a healthy spleen in children change all the time (in full accordance with the age and size of a continuously growing body). The average indicators of organ sizes for children belonging to different age categories are indicated in the list:
Based on the data in the list, it is possible to establish whether the size of the spleen obtained during its ultrasound examination corresponds to the age norm. In case of discrepancy between the indicators, the doctor may suspect the presence of:
Spleen palpation methods
When performing a superficial examination of the area of \u200b\u200bthe left hypochondrium, it is necessary to pay special attention, since even a slight increase in this organ allows one to grope for a rather dense cone-shaped formation located at the edge of the costal arch. If the patient has splenomegaly (a pronounced enlargement of the spleen), provoking the bulging of most of it from under the edge of the costal arch, there is no need to perform deep palpation, since in this case, superficial probing is quite enough. Since palpation of the spleen, carried out with an upright position of the patient, in most cases seems difficult due to the strong tension of the abdominal muscles, it is carried out:
And in fact, and in another case, the palpation technique is subject to the same principles. The position of the patient on the side, contributing to a good relaxation of the muscles of the left half of the abdomen and a slight displacement of the examined organ downward, is more suitable for palpation. At the same time, this position is associated with some inconveniences for the doctor. To feel the spleen, he must either squat down on the couch, or kneel down next to it.
The doctor places the brush of the right (palpating) hand flat on the left side of the abdomen so that its base is turned towards the pubis, and the terminal phalanges of the closed and slightly bent fingers are located at the same level at the very edge of the costal arch (left). The terminal phalanx of the middle finger should be located in the corner formed by the lower edge of the tenth rib and the tip of the eleventh rib. The thumb of the right hand does not take part in this manipulation. The left hand is placed on the left side of the patient's chest along the seventh to tenth ribs at the level of the anterior axillary (axillary) line. Her fingers should be turned towards the spinal column. During respiratory movements, the doctor's left hand should slightly limit the lateral movements of the costal arch, creating conditions for increasing the respiratory excursion of the diaphragm, which contributes to the downward displacement of the spleen. In the process of palpation, the researcher performing it regulates the patient's breathing. If, during percussion or superficial palpation, information was obtained about the localization of the lower border of the spleen, the fingers of the palpating hand are set one or two centimeters below it. After that, the doctor makes a skin fold, displacing the skin of the anterior abdominal wall by three to four centimeters in the direction opposite to the costal arch. Thanks to this technique, the doctor creates a reserve of skin under his fingers, which facilitates their smooth movement deep into the left hypochondrium. Following this, the patient exhales, and the specialist performing palpation, along with lowering the abdominal wall, gently plunges the fingers of the right hand into the abdominal cavity (at an angle of 35-45 degrees), leaving the hand in this position until the end of the next inhalation. The space left between the dorsum of the hand and the costal arch should be sufficient to allow passage of the lower pole of the spleen. Having invited the patient to make a deep and unhurried breathing movement with the abdomen, the doctor presses the left costal arch with the fingers of his left hand, somewhat limiting its mobility. At this moment, the fingers of the palpating hand, being motionless, remain in the depths of the abdominal cavity, opposing the pushing movement of the abdominal wall. At the moment of inhalation, the left dome of the diaphragm descends, displacing the spleen downward, as a result of which it falls into an artificially created pocket. During exhalation, the organ returns to its original position. It is this moment, when the spleen slides over the fingers, that the doctor uses to assess its condition and quality. Sometimes the spleen may not get into the pocket, just touching its lower edge with the terminal phalanges of the fingers. In such cases, a specialist who seeks to feel this organ should, during inhalation, slightly push the palpating hand forward, straightening the fingers, making them either stroking (from above) or prying (from below) movements. It must be remembered that careless palpation is fraught with damage to this extremely vulnerable organ.
Lying on its side, the patient should turn to the right side (at an angle of 45 degrees) to the surface of the couch, placing his folded palms together under the right cheek. The patient's right leg should be extended, and the left leg, in order to relax the abdominal muscles, should be bent at the knee joint and slightly brought to the torso. The specialist can take the usual position, but if there is a too low couch and insufficient flexibility of the wrist joints, he will have to perform palpation while squatting or kneeling in front of the bed on his right knee. It is this position that allows his right hand to lie flat on the patient's stomach. The further method of palpation of the spleen according to Sali practically does not differ from the above-described method of bimanual examination of it, carried out in the position of the patient lying on his back.
Splenomegaly allows us to grope on the front edge of the organ of interest to us for the presence of characteristic cutouts that are absent in the kidney, endowed with a number of specific features inherent only to it.
The specialist performing the manipulation, with the terminal phalanges of the fingers of the palpating hand, brought together and slightly bent, performs a series of short, abrupt and jerky blows on the anterior abdominal wall (the fingers do not come off the surface of the skin). The direction of the applied shocks, taken with the aim of bumping into the test organ, should be perpendicular to its expected lower edge. At the very beginning of the study, the specialist begins to apply jerky blows on the left side of the abdomen at the level of the anorectal (scallop) line of the anal ring, gradually moving the fingers to the costal arch. This movement continues until there is a sensation of collision with a solid body, while extending deep into the abdominal cavity, and then floating up and again hitting the end phalanges of the researcher's fingers. This phenomenon is called the "floating ice" symptom. It is at the moments of such collisions that the surface of the examined organ is felt. The video shows the technique of palpation of the spleen:
Norms and pathologiesThe spleen, which takes part in the formation of the immune system, in the fight against pathologies of the bone marrow and blood, in all types of carbohydrate and lipid metabolism, plays a very important role in the human body. That is why even minor disruptions in the work of this body (and even more an increase in its size) are grounds for serious concern. In these cases, the patient is referred for ultrasound examination. The indicator of the norm is:
Signs of pathology can be presented:
The detection of even minor deviations from the standard parameters is of great diagnostic value, requiring the obligatory consultation of a qualified specialist. The spleen is located deep in the left hypochondrium, lateral to the stomach. It is located directly under the left dome of the diaphragm and therefore, like the liver, has respiratory mobility. The spleen has an ovoid shape and is projected onto the left lateral surface of the chest between the IX and XI ribs, and the length of the organ approximately corresponds to the course of the X rib. The method of palpation of the spleen is basically the same as that of the liver. Palpation is performed initially with the patient lying on his back. The palm of the palpating right hand is placed in the left flank of the abdomen outward from the edge of the rectus muscle so that the base of the palm is directed towards the pubis, and the tips of the closed and slightly bent fingers are at the same level at the edge of the left costal arch. In this case, the tip of the middle finger should lie in the corner between the lower edge of the X rib and the free end of the XI rib. The thumb of the right hand is not involved in palpation. The palm of the left hand is placed in the transverse direction on the lateral part of the left half of the chest along the costal arch in order to restrict lateral movements during breathing during palpation and create conditions for increasing respiratory excursions of the left dome of the diaphragm, and, accordingly, the spleen. During palpation, the doctor regulates the patient's breathing. First, the doctor offers the patient to inhale with the "stomach", and at this time, with the fingers of his right hand, he displaces the skin of the abdominal wall by 3-4 cm in the direction of the palm, i.e. to the side opposite to the costal arch. This creates a reserve of skin under the fingers to facilitate their further advance into the depths of the abdominal cavity. After that, the patient exhales, and the doctor, following the descending abdominal wall, smoothly plunges the fingers of the right hand deep into the abdomen and fixes the hand in this position until the end of the next inhalation. There should be enough space between the costal arch and the dorsum of the fingers to allow the lower pole of the spleen to pass. Then the patient is again offered to breathe deeply with the "stomach". At this time, the doctor presses with his left palm on the left costal arch to limit its mobility, and holds the fingers of the right hand motionless in the depths of the abdomen, resisting the pushing movement of the abdominal wall (Fig. 61). On inspiration, the diaphragm descends and its left dome pushes the spleen down. If the spleen is accessible for palpation, its lower pole, while descending, penetrates between the fingers and the costal arch into the pocket formed from the pressure of the fingers on the abdominal wall, and then, sliding out of it, bypasses the fingertips and thus palpates. Sometimes the spleen does not enter the pocket, but only bumps its lower pole against the tips of the fingers. In this case, in order to feel it, it is necessary to move the right hand forward while inhaling, straightening the fingers in the bent phalanges and making them stroking from above or prying from below (as with palpation of the liver) movements. However, the spleen should be palpated very carefully so as not to damage it.
The study is repeated several times, and in addition, palpation is performed in the position of the patient on the right side (according to Sali). In this case, the patient's right leg should be straightened, and the left leg should be bent at the knee and slightly brought to the body. The patient places both his hands, folded together, under the right cheek. The doctor goes down by the bed on his right knee and palpates the spleen using the same techniques as for palpation in the supine position of the patient (Fig. 62). When the spleen is found, the degree of its enlargement, consistency, surface nature, and the presence of pain are determined. Normally, the spleen is not palpable. If you can feel it, then it is increased. With a pronounced increase in the spleen (splenomegaly), a significant part of it protrudes from under the costal arch and can be examined by superficial palpation without using the described method of deep palpation. In order to distinguish an enlarged spleen from an enlarged kidney, it is necessary to additionally carry out palpation in a standing position: the spleen then moves backwards and its palpation is difficult, and the kidney goes down and therefore becomes more accessible for palpation. In addition, with splenomegaly, characteristic notches are palpated at the anterior edge of the spleen, while the kidney, when palpated, has its own specific features. After palpation of the spleen, its percussion dimensions are determined according to Kurlov. To do this, first find the upper and lower borders of the spleen, and then its anterior and posterior edges. The study is carried out in the position of the patient lying on the right side, as with palpation according to Sali. The finger plessimeter is placed parallel to the defined border of the organ. Percussion is carried out from the area of \u200b\u200ba clear (tympanic) sound to a more dull one, using quiet percussion strikes. After each pair of blows, the finger-pessimeter is shifted by 0.5-1 cm. The found boundary is marked along the edge of the finger-plessimeter, facing towards a clear (tympanic) sound. It should be borne in mind that with the normal size of the spleen, it is not a dull, but a moderately dull percussion sound with a tympanic shade that is determined above it due to the close location of the air "bubble" of the stomach (Traube space) and intestines containing gas. First, the upper and lower borders of the spleen are determined. For this, the finger-plessimeter is installed in the transverse direction on the left lateral surface of the chest at the level of the V rib. The middle phalanx of the finger should lie on the mid-axillary line and be perpendicular to it. Percussion along this line along the ribs and intercostal spaces, maintaining the transverse position of the finger-pessimeter, in the direction of the wing of the left iliac bone until the border of the transition of a clear pulmonary sound to a dull one is detected. This border corresponds to the upper border of the spleen and is normally located on the IX rib (the ribs are counted from the free end of the XII rib).
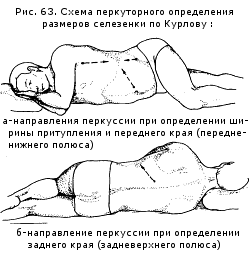
Marking the found border with a dermograph or fixing it with the little finger of the left hand, set the plessimeter finger directly above (proximal) the wing of the left iliac bone and percussion along the mid-axillary line in the opposite direction (Fig. B3a). The border of the transition of tympanitis into a dull sound corresponds to the lower border of the spleen and normally lies on the XI rib. The distance between the upper and lower borders of the spleen is measured. Normally, it is 4-7 cm and is called dull width. When determining the anterior edge (antero-inferior pole) of the spleen, the pessimeter finger is placed longitudinally along the anterior midline of the abdomen so that the middle phalanx of the finger is on the umbilical line and is perpendicular to it. Percussion in the direction of the spleen along the line connecting the navel and the point of intersection of the X left rib with the middle axillary line (Fig. 63a). The border of the transition of the tympanic sound to the blunt one corresponds to the anterior edge of the spleen. Normally, it does not go beyond the anterior axillary line. To determine the posterior edge (posterosuperior pole) of the spleen, it is necessary to first feel the left X edge and find its posterior end at the spine. Then a finger-pessimeter is installed along the left paravertebral line so that its middle phalanx lies on the X edge and is perpendicular to it. Percussion along the X rib in the direction of the spleen, keeping this position of the finger-pessimeter (Fig. 63b). The transition of a tympanic sound to a dull one corresponds to the posterior edge of the spleen. Mark this place with a dermograph. Normally, the posterior edge of the spleen does not protrude beyond the left scapular line. By measuring the distance between the anterior and posterior edges of the spleen, they find the length of dullness, which is normally 6-8 cm. With a significant increase in the spleen, its anterior edge can protrude from under the costal arch. In this case, the protruding part of the spleen is additionally measured. You can also use another simple way to detect an increase in the size of the spleen. So, if in the position of the patient on the right side (according to Sali) during percussion at the intersection of the X left rib with the middle axillary line, a dull sound is detected, similar to a percussion sound over the liver, this indicates a significant increase in the spleen (Ragoza symptom). An increase in the size of the spleen is an important diagnostic sign of a number of pathological processes. In particular, an enlargement of the spleen in combination with an increase in the size of the liver and peripheral lymph nodes is determined in some acute and chronic infections, sepsis, infective endocarditis, hematological malignancies and systemic immunopathological diseases. A simultaneous increase in the size of the spleen and liver is observed in patients with chronic active hepatitis, liver cirrhosis, hemolytic anemia, storage diseases (Gaucher, Niemann-Pick). An isolated enlargement of the spleen can be caused by thrombosis of the splenic or portal vein, the development of a tumor, cyst, and other local pathological processes in the spleen. In acute infectious diseases and septic processes, its consistency is soft, test, while in chronic infections, liver cirrhosis, leukemia, and especially in amyloidosis, it is usually compacted. The most pronounced enlargement of the spleen is observed in a special form of chronic myeloid leukemia - osteomyelofibrosis. In this condition, the spleen sometimes occupies most of the abdominal cavity. Soreness of the spleen can be associated with a rapid increase in its volume, leading to stretching of the capsule, or with perisplenitis. The tuberosity of the surface most often indicates a previous infarction of the spleen, but sometimes it is a consequence of its echinococcosis, syphilis, abscess, cystic or tumor lesions. Palpation of the liver and spleen with ascites is often difficult. In this case, palpation of the liver using the described method of deep palpation should be additionally carried out with the patient lying on the left side and standing with a slight forward tilt of the trunk, and it is better to palpate the spleen while lying on the right side (according to Sali). With severe ascites, the method of ballot palpation is used to detect hepato- and splenomegaly. The study is carried out with the patient lying on his back. The doctor, with the tips of the closed and slightly bent fingers of his right hand, without tearing them off the skin, applies short abrupt jerky blows to the anterior abdominal wall perpendicular to the supposed lower edge of the organ under study, trying to bump into it. In this way, he begins to apply pushes along the corresponding half of the abdomen at the level of the scallop line and gradually moves the fingers in the direction of the costal arch until a sensation of impact on a solid body is obtained, which at the same time departs into the depth of the abdominal cavity, and then floats up and hits the fingertips again (symptom " floating ice "). At this point, the surface of the organ can be felt. In the process of deep palpation of the abdominal organs, it is sometimes possible to identify additional pathological formations, in particular a tumor or cyst. In these cases, it is necessary to determine the exact localization of the palpable formation in the abdominal cavity, its shape, size, consistency, the presence of fluctuations, the nature of the surface, mobility (displacement), communication with neighboring organs, pain. A mass directly associated with the anterior abdominal wall is usually noticeable already on examination. It is palpable both during relaxation and tension of the abdominal muscles, and during respiratory excursions of the abdomen it moves in the anteroposterior direction along with the abdominal wall. Intra-abdominal formation is visually determined only if it is large enough. With an arbitrary tension of the abdominal muscles, palpation of the intra-abdominal formation is difficult, and when the muscles of the abdomen are relaxed, the mobility of such a formation and its movement in the upper-lower direction during breathing can be detected. However, it should be borne in mind that the displacement of an intra-abdominal formation depends on the natural mobility of the organ from which it originates, and, if this formation is a tumor, then on the presence of germination into neighboring organs. The retroperitoneal formation is deeply located in the abdominal cavity and is closely connected with its posterior wall. It is inactive and, as a rule, is covered by the organs of the abdominal cavity, for example, the intestine or stomach. The spleen is located normally under the left dome diaphragm in the lateral part of the left hypochondrium, adjacent to the chest wall between the IX and XI ribs. Its longitudinal axis runs in an oblique direction, parallel to the X edge. A patient with spleen percussion should be in a horizontal position, lying on the right side, the left arm should be bent at the elbow joint and lie freely on the front surface of the chest, the right arm should be under the head, the right leg is extended, the left arm should be bent at the knee and hip joints. Quiet percussion is used. First, the upper and lower borders of the spleen are found, then the anterior and posterior. To determine the upper border, the finger-pessimeter is placed in the 4th or 5th intercostal space along the mid-axillary line and percussion is performed from top to bottom until a dull sound appears. The border is marked on the upper edge of the plessimeter finger, facing the clear sound. The lower limit is also determined along the middle axillary line, placing a finger-pessimeter under the XII rib and percussion from bottom to top until dull. To determine the anterior border of the spleen, the finger-pessimeter is placed on the anterior abdominal wall, to the left of the navel, parallel to the desired border (approximately at the level of the X rib) and percussed towards the diameter spleen before dullness appears. The mark is placed on the side of the clear sound. Normally, the anterior border is 1–2 cm to the left of the anterior axillary line. To find the posterior border of the spleen, percussion is performed along the X edge, setting the finger-pessimeter perpendicular to it. Percussion begins between the scapular and posterior axillary lines and is percussed from back to front until a dull sound appears. Next, measure the distance between the upper and lower boundaries of the spleen, i.e. the diameter, which is located between the IX and XI ribs and is normally 4-6 cm. Then measure the distance between the anterior and posterior borders of the spleen, i.e. the length of the length, which is normally 6-8 cm.Normally, the spleen is not palpable, since it is located deep in the left hypochondrium, not reaching the edge of the costal arch by 3-4 cm.Therefore, a successful palpation of the spleen indicates either its enlargement or prolapse ... Palpation should be carried out in two positions of the patient - on the back and on the right side. The principle of palpation is the same as for the liver. The first point is setting the hands. The left hand is placed flat on the lower part of the left half of the chest to delimit its outward movements during inhalation and to increase the downward displacement of the diaphragm, and with it the spleen. The right hand with slightly bent fingers is placed on the anterior abdominal wall parallel to the costal edge, opposite the X rib. The second and third point is the formation of an artificial pocket according to V.P. Obraztsov. To do this, on exhalation, it is necessary with a superficial movement to pull the skin down towards the navel and immerse the fingertips of the right hand into the depth of the abdominal cavity while moving them towards the left hypochondrium. The fourth point is palpation of the spleen. The subject is asked to take a slow and deep breath. The edge of the spleen, going down under the pressure of the diaphragm, reaches the fingertips, creating a moment of tactile sensation. If it is not possible to feel the spleen, the fingers are moved towards the edge of the costal arch by 1-2 cm. The study is carried out until the digital phalanges of the right hand feel the spleen or the edge of the costal arch. A characteristic feature of the spleen is the presence of 1 to 3 notches on its front edge, which makes it possible to distinguish an enlarged spleen from other formations. |






 Palpation (probing) is one of the main methods of examining the spleen.
Palpation (probing) is one of the main methods of examining the spleen.

New
- Confused consciousness: symptoms, causes and treatment
- Laparoscopy (removal) of appendicitis
- The liver is not palpable what does it mean Determination of dimensions according to Kurlov
- Pathological types of bite and methods of their correction Tests for determining bite anomalies
- Cancer stages International tumor classification
- Inflammation of the appendages in women - symptoms and treatment regimen
- Thyroid disease in women
- Examination of the spleen. Palpation of the spleen. Spleen palpation technique Spleen along the costal margin
- All about follicles in the ovaries
- The superior vena cava is formed from the fusion of veins




