Site sections
Editor's Choice:
- Is a single kidney pregnancy possible?
- Varnish for stone with a wet effect
- How an optometrist checks eyesight
- How to take grape oil
- Getting a driver's license: restrictions on vision
- Skin care at home
- Inexpensive personal care products
- How to get margarine and how to choose it correctly?
- How to speed up cervical dilatation before childbirth
- Peonies do it yourself: do it together
Advertising
| How dangerous is living with one kidney. Is a single kidney pregnancy possible? |
|
15-20 years ago, our medicine categorically denied the possibility of normal pregnancy and vaginal pregnancy in renal or cardiac pathologies. However, today a single kidney pregnancy is no longer a big challenge for modern doctors. Although some of them do not cease to be reinsured and categorically do not recommend giving birth with such a renal anomaly. In the material below, we consider whether a woman has the chance to bear and give birth to a healthy baby without risk to her own health if there is only one kidney.
Functions of the urinary organsThe kidneys are exclusively the paired organ of the human excretory system. They are located in the retroperitoneal space on two sides of the spine. Localization of organs is noted in the region of 11–12 vertebrae of the thoracic and 1-2 vertebrae of the lumbar. The main function of the kidneys is excretion. That is, they remove (excrete) toxins, poisons and metabolic products from the body along with urine. During the day, blood plasma passes more than 60 times through the nephrons (the structural unit of the urinary organs), clearing everything that is unnecessary there. Then plasma and blood are returned to the human circulatory system, and all toxins and poisons follow into the renal pelvis system and then go out with the urine. Needless to say in this case that the loss of one paired organ significantly loads the second remaining one. That is, the second kidney works for two.
In addition, in addition to the excretory function of the kidneys and perform these:
It is a little about a removed (absent) kidney and a condition of an organism at the same time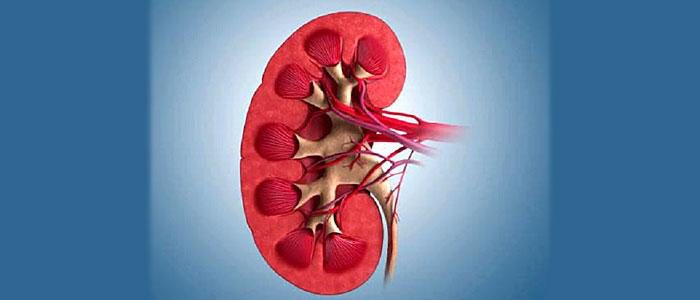 It is worth knowing that the absence of a paired organ in the body can be either congenital or acquired. At the same time, the human body with agenesis (congenital absence of the second kidney) already from birth automatically learned to work in this mode, while the removal of a kidney, according to indications, forces all systems to rebuild to work with one kidney for almost 2 years. That is why women who have one of them removed have been advised to plan a pregnancy no earlier than 2 years later. So much time is left for the rest of the body to use the backup nephrons for high-quality blood purification. We also note that the second kidney increases in size, taking on the load of the removed organ. Here, at the time of compensation, she becomes inflamed until her compensatory abilities normalize the work of the excretory system.
The reasons for kidney removal can be:
Possible difficulties in pregnancy with one kidney
Possible complications of carrying a fetus against the background of a single kidney depend on the reasons for which the first organ was removed. This is due to the fact that the body could undergo a serious load on the immune system, depending on the pathology leading to nephrectomy (removal of the organ). So, the causes and possible consequences of the removal of the kidney for the future mom:
General positive information for women with one kidneyModern medicine claims that it is possible to bear a pregnancy and even give birth naturally to women with one kidney. However, the condition requires constant monitoring. It should be understood that there is still a certain proportion of risk for a patient with one organ and for the fetus. Therefore, you need to be prepared for the fact that caesarean section will be used to resolve the pregnancy in order to preserve the kidney.
The compensatory capabilities of paired organs are such that the absence of one of them does not prevent the implementation of the basic functions of the body. Currently, it is safe to say that pregnancy develops normally in women with one ovary, one adrenal gland, one lung or one kidney. A single kidney is a congenital developmental abnormality or the consequence of the removal of another kidney affected by the pathological process. In the second case, the adaptation period proceeds in 2 stages. At first, there is a relative functional insufficiency of the organ, since the function of the remaining kidney has not yet increased significantly; there is a loss of functional reserve, since all nephrons are functioning; hyperemia of the kidney appears and its hypertrophy begins. At the second stage, there is full functional compensation characterized by an increase in kidney function, restoration of the functional reserve, moderate but stable hyperemia and hypertrophy increasing to a certain limit. The reserve capabilities of the kidney are mobilized from the first days after nephrectomy and are aimed primarily at removing water and sodium chloride. Nitrogenous slags are not fully excreted, but this is beneficial because, accumulating in the blood, nitrogenous substances stimulate compensatory renal hypertrophy. Morphological and functional hypertrophy of the glomerular tubular apparatus occurs. Compensation of the function of a lost kidney is completed 1-1.5 years after nephrectomy . The large reserve capacity of the kidney can be judged by the fact that normally only 1/4 of the nephrons function simultaneously. After nephrectomy, the blood flow in the kidney increases by 1.5 times, and its functional ability is maintained at the level of the needs of the body. Women with one kidney can not be considered completely healthy, their kidney has a limited reserve of functional activity. The nephrons of the remaining kidney are forced to carry a double load, and therefore their functional failure can occur over time. Therefore, the most favorable period for pregnancy occurs through2 years after nephrectomy, when the functional restructuring of the organ is completed, and the reserves of the kidney are not yet exhausted. This can be established by examining a woman in the first trimester of pregnancy. With one kidney, the renal blood flow and glomerular filtration increase to the same extent as in healthy women with two kidneys. The physiological functions of the remaining kidney during pregnancy are usually normal, the excretory function is not impaired. Blood pressure is not elevated, proteinuria is absent, and urea clearance is normal. The condition of a woman during pregnancy depends on the reason for the removal or absence of one kidney. A congenital, only ectopically located kidney copes with its functions worse than a healthy normally located kidney remaining after the removal of its pair. If the cause of nephrectomy was pyonephrosis, tuberculosis or urolithiasis, then the woman's condition improves, since the source of intoxication of the body is eliminated along with the kidney. It is not so important which kidney is removed, although the prognosis for pregnancy is better with right-sided nephrectomy, since the right kidney and ureter are more likely to undergo changes during pregnancy. Women who have undergone nephrectomy are more likely to suffer from pyelonephritis during pregnancy; it is possible that latent disease is activated. However, according to our observations, kidney function suffers little; it does not deteriorate significantly during pregnancy or after childbirth. Late toxicosis, for unclear reasons, rarely develops in women with one kidney. A little more often occurs polyhydramnios and weakness of labor. Babies are born healthy, with normal body weight and height. Perinatal mortality is less than 100%. The most unfavorable obstetric prognosis in women with congenital aplasia of one kidney. A single kidney may not be completely functionally complete, although this was not manifested before pregnancy. During pregnancy with anomalies of urinary tract development, including kidney aplasia, pyelonephritis often occurs, perinatal mortality and the frequency of birth of immature children significantly increase. Often there is a combination of abnormal development of the genital and urinary organs. Detection of some (usually on the one hand) defects in the structure of the genital organs (one-horned uterus, etc.) gives grounds to suspect anomalies of development of the urinary organs on the same side. However, to prove the presence of congenital pathology of the kidneys and ureters, includingand absence of a kidney, without radiological examination is not possible. Births in women with congenital aplasia of the kidney proceed safely. However, if the kidney is located in the pelvis, the fetus may assume an abnormal position; in this case, a cesarean section becomes necessary. In the case of pregnant women with one kidney, tuberculosis was the most common cause of nephrectomy. Apparently, in the future, this group of women will be reduced, since in recent years, conservative methods of treating kidney tuberculosis have prevailed. After nephrectomy for bladder tuberculosis in another kidney, residual effects caused by intoxication (toxic effects of kidney tuberculosis or specific cystitis) may persist. Intensive anti-tuberculosis therapy, against which nephrectomy is performed, eliminates intoxication within a few months. However, before postoperative complications and intoxication disappear, pregnancy should not be resolved. Pregnancy is permissible if the causative agent of tuberculosis has not been detected in the urine for several years after the operation, there are no specific changes in the urinary tract and the woman does not need treatment for tuberculosis (removed from the register in the tuberculosis dispensary). We have given birth to women twice. Because tuberculosis affects not only the kidneys, it is necessary to make sure that there is no specific process in other organs. For this, besides careful Learn the history and physical examination should obtain the opinion of a doctor, a TB TB dispensary. If the kidney is preserved after nephrectomy forhydronephrosis, it is not affected by the same disease, its function during pregnancy remains sufficient, and pyelonephritis rarely joins. Other observations that exist in the literature relate, it must be said, to cases of nephrectomy with bilateral hydronephrosis. Hypertension, renal failure, pyelonephritis may appear in such patients during pregnancy. Great care is required when deciding on the acceptability of pregnancy in women who have undergone nephrectomy for pyelonephritis. The remaining kidney can be perfectly healthy, and then the pregnancy proceeds safely. Most of these observations. But the inflammatory process in the kidney can occur latently, without being detected in time and subjected to treatment, it threatens with an exacerbation during pregnancy, which is not always amenable to conservative therapy. This also applies to women with pronounced pyelonephritis of a single kidney, the condition of such patients, as a rule, worsens during pregnancy. This affects both the course of pregnancy and the health of the fetus, leading to azotemia, premature birth, malnutrition or fetal fetal death. Pregnancy in women after nephrectomy forkidney diseaseusually proceeds normally. The condition may worsen with the presence of stones or pyelonephritis of a single kidney. Successful diagnosisand treatment renovascular hypertensionled to the emergence of pregnant women whose kidney was removed due to this disease. Renovascular hypertension is caused by damage to the stenosing process of the renal artery or its branches. The decrease in renal blood flow is the trigger of the renin-angiotensin-aldosterone hypertensive system. The only radical treatment for such patients is surgery (reconstructive surgery on the renal artery or nephrectomy). After surgery, high and stable blood pressure normalizes fairly quickly. Our watchthis shows that if pregnancy occurred in a yearand more after nephrectomy, when blood pressure is normal, and the kidney is adapted to the changed conditions of functioning, the gestational period is uneventful. If pregnancy occurs in the first months after surgery, it often ends in a spontaneous abortion. Pregnancy and childbirth after removal of a kidney affected by a tumor are rarely found. Only 20% of women live longer than 5 years, since 80-85% of kidney tumors are malignant. Kidney tumors often recur. The prognosis for pregnancy is unfavorable. Pregnancy is contraindicated. Only in some cases it is permissible if more than 5 years have passed since nephrectomy and no tumor recurrence has been detected. Whatever the cause of nephrectomy, the possibility of preserving pregnancy depends primarily on the condition of the remaining kidney. Therefore, it is necessary to thoroughly check the ce function (excretory, concentration, filtration). The most thorough examination of pregnant women with one kidney, which we carried out, includes, in addition to the specified minimum of tests, also a study of the cardiovascular system (ECG, general hemodynamic parameters, condition of the fundus vessels) electrolytes in plasma and urine, the acid-base state of the blood, total protein and protein fraction of the blood, indicators of renal hemodynamics and kidney function showed that 2/3 of women have significant disturbances eniya absent. Only in individual patients were signs of pronounced impairment of the function of the remaining kidney. In every patient with one kidney, it is imperative to ascertain the presence of a urinary tract infection. Pyelonephritis significantly worsens the prognosis of the disease and questions the possibility of pregnancy. We have diagnosed pyelonephritis in 15% of pregnant women who underwent nephrectomy. Other researchers found it much more often. If nephrectomy was due to kidney tuberculosis, a urinalysis should be done for the presence of mycobacterium tuberculosis. The absence of one kidney does not affect the duration of pregnancy. All women observed by us were giving birth in a timely manner, with the exception of the few cases when they were caused prematurely due to the severity of the patients' condition. Delivery and cesarean section in all women was uneventful. The postpartum period is rarely complicated by endometritis or deterioration of the organs of the urinary organs. In conclusion, it should be noted that in most women with one congenital kidney or undergoing nephrectomy, pregnancy and childbirth can occur without affecting their health. Repeated delivery does not worsen the condition. Pregnancy is contraindicated if kidney function is sharply reduced, especially in the presence of azotemia or arterial hypertension, as well as in case of tuberculosis and pyelonephritis of a single kidney. If you find an error, please highlight a piece of text and click Ctrl + Enter. If a woman has one kidney after surgery or a birth defect, is it worth getting pregnant at all and what is the chance to bear and then give birth to a healthy child? What does medicine say?The loss of any one pair of internal organs is compensated by strengthening the functions of the remaining one. And the kidneys are no exception! If one kidney is removed, thanks to the compensatory properties, the second after a year and a half almost approaches the level of functioning of two kidneys. Today, doctors say that a woman who lives with one kidney is able to bear and give birth to a healthy child, but subject to constant medical supervision of the entire pregnancy by a gynecologist and a urologist. Even considering that during pregnancy the volume of the liquid part of the blood increases significantly, which affects the amount of urine, the only kidney is able to cope with such a load. The absence of a kidney does not affect miscarriage, its duration or preterm labor. What should the expectant mother know in this case?Before allowing a woman with one kidney to give birth, doctors take into account many circumstances, because you cannot consider such women fully healthy. After removal of one kidney, the remaining organ works with double load, which is fraught with gradual functional depletion. Even in the absence of signs of damage to the second kidney, such people have a limited reserve of functional activity, and with an increase in load, one kidney cannot compensate for the function of two. The consequence may be latent renal failure. The most favorable period to get pregnant with one kidney is 2-4 years after the operation, when the functional reorganization of the organ has already been completed. Then, during pregnancy, the function of the remaining kidney is usually normal. With one kidney pregnancy and childbirth directlydepend on the success of the operation and the state of the body after it. Women with a remote kidney are more susceptible to complications. In the first place - as well as preeclampsia - severe complication of pregnancy associated with protein in the urine, increased pressure and edema. The significance of the reason for the removal of the kidney. If it is a kidney disease, purulent process, kidney tuberculosis, then elimination of the source of intoxication improves the functioning of the kidney after surgery, ensuring a successful pregnancy and childbirth. The success of pregnancy in removing a kidney for hydronephrosis ensures good function of the remaining kidney, and pyelonephritis (even severe) - a healthy remaining kidney. If it is infected, the prognosis worsens. Dismal prognosis for a single congenital kidney. She often has changes in the structure and location, more prone to disease. In such women, pregnancy often does not occur, and when it occurs, urinary tract infections are frequent, the risk of birth of immature children, fetal or newborn mortality is increased. Pregnancy is not desirable when a kidney is removed due to a tumor. In this case, the oncologist determines the prospects of pregnancy, taking into account the characteristics of the tumor, the woman’s age, the time elapsed after the operation. Pregnancy is contraindicated in one kidney in case of a sharp decline in its function.especially with renal failure. The definition of “single kidney” includes not only the congenital absence of a kidney, but also the loss of the function of one of the kidneys as a result of a disease (pyelonephritis, hydronephrosis, urolithiasis, tumors, injuries). ICD-10 software code EPIDEMIOLOGYCongenital absence of one kidney is not a very rare anomaly, occurring, on average, in one case in 1800–2000 urological patients. The proportion of nephrectomies performed for malignant diseases leaves only 10–12% of the total number of surgeries. ETIOLOGYA single kidney may be a congenital developmental abnormality or remains after the removal of the second kidney for any disease: hydronephrosis, pyelonephritis, nephrolithiasis, kidney tuberculosis, renovascular hypertension, tumors, injuries, etc. In the absence of pathological processes in the congenital single kidney, this anomaly often remains unrecognized during pregnancy and is detected when a disease is affected. PATHOGENESISCompensatory reorganization of the only kidney remaining after nephrectomy proceeds in two stages. · The first stage is characterized by relative functional insufficiency of the organ (the function of the remaining kidney has not yet significantly increased), loss of the functional reserve (all nephrons are functioning), acute hyperemia of the kidney and incipient hypertrophy. · The second stage is characterized by: complete functional compensation (the kidney function is doubled), restoration of the functional reserve (part of the nephrons is not functioning), moderate but stable hyperemia and hypertrophy increasing to a certain limit. From the first day after nephrectomy, the remaining kidney mobilizes its reserve forces, and, above all, its adaptation to the removal of water and sodium chloride occurs. Nitrogenous substances, accumulating in the blood, serve as an initiating factor for the development of compensatory hypertrophy of the kidney. There is hypertrophy of the glomerular and tubular zones, and not only voluminous, but also functional. The reserve capacity of the kidney is great. Normally, only 1/4 of the renal parenchyma functions simultaneously. After nephrectomy, the blood flow of the remaining kidney increases by 30–50% and its functional ability is maintained at close to normal levels. The functions of a lost kidney are compensated for a long time. Some authors believe that compensation is completed only 1–1.5 years after the operation. As a result of the elimination of one kidney, the load on the remaining nephrons doubles, the intense activity of which gradually leads to the functional depletion of the remaining organ. According to urologists, individuals who have undergone nephrectomy cannot be considered completely healthy even when they have no signs of lesion of the remaining kidney. A single kidney cannot fully take over the functions of the two. The reserve capacity of one kidney is limited, and it is sensitive to various endo and exogenous effects. PATHOGENESIS OF GESTATION COMPLICATIONSPregnancy and childbirth in the presence of a single kidney are quite possible. In deciding whether pregnancy is possible, the age of the patients, the nature of the disease about which the nephrectomy was performed, and the age of this operation are taken into account. To complete the vicarious processes in the remaining kidney, an average of 1.5–2 g is needed. The course of pregnancy and childbirth can be favorable after kidney removal for nephrolithiasis, tuberculosis and hydronephrosis. Pregnancy and childbirth after removal of a kidney affected by the tumor are rare. With malignant tumors, the 5-year survival rate of women is 20%, with benign tumors - almost 80%. Pregnancy can be maintained, provided that no tumor recurrence has been detected for 5 years after nephrectomy. Pregnancy in women after nephrectomy due to urolithiasis usually proceeds normally. A woman’s condition during pregnancy can worsen with nephrolithiasis or pyelonephritis of a single kidney. In recent years, the number of women undergoing nephrectomy has been increasing, including due to patients in whom the kidney has been removed due to renovascular hypertension. The etiological factor of renovascular hypertension is a stenosis of the renal artery and its branches, which has developed as a result of developmental anomalies or various diseases. Narrowing of the renal artery activates the reninangiotensin-aldosterone system, the main pathogenetic factor of renovascular hypertension. After surgery (reconstructive surgery on the renal artery or nephrectomy), the blood pressure normalizes rather quickly. Pregnancy with this disease is possible no earlier than 2 years. In women with a single kidney, preeclampsia does not develop more often than in the population. The frequency of spontaneous abortions does not increase. Children are usually born healthy, with a normal weight and body length. PS slightly exceeds the average in the population. CLINICAL PICTUREPregnancy and childbirth in a clinically healthy single kidney proceed safely. COMPLICATIONS OF THE GESTUREIn the first trimester, the threat of termination of pregnancy, in the third trimester, preeclampsia and the threat of premature birth, which do not exceed the average population indicators. DIAGNOSTICSSCREENINGAll pregnant twice a month pass a complete urinalysis. ANAMNESISA history of congenital abnormality of development or removal of the second kidney due to a disease: hydronephrosis, pyelonephritis, urolithiasis, tuberculosis of the kidney, renovascular hypertension, tumors, trauma, etc. PHYSICAL SURVEYIt is necessary to check the symptom Pasternatskiy. LABORATORY RESEARCH· Clinical blood test. Regardless of the cause of nephrectomy, the question of preserving pregnancy is decided on the basis of the functional state of the remaining kidney. Therefore, conduct a thorough study of the functions of the kidney (excretory, concentration, nitrogen-secreting ability, glomerular filtration). TOOL RESEARCH· Ultrasound of the kidney. · Doppler sonography of the kidney. · Liquid crystal thermography. · Thermal imaging method (thermography). The functional state of an organ (kidney) is reflected in its temperature. This is due to the fact that the biochemical processes in the body (organs, tissues, cells) are manifested by appropriate temperature reactions. Thermography allows visually and measuring (with a high accuracy of 0.01 ° C / mm2) to estimate the infrared (thermal) radiation from the surface of the body, where temperature influences from internal structures extend. The method allows to evaluate the functional changes in the dynamics, i.e. follow the changes during the treatment. · Ureteral catheterization. · Chromocytoscopy. The patient is intravenously injected with 5 ml of a 0.5–10% solution of indigo carmine, and then the time of appearance of urine-stained urine-colored urine from the mouths of the ureters is recorded through a cystoscope. In a healthy person, colored urine begins to separate from the ureter 3–5 minutes after the injection of dye. With the defeat of one of the kidneys, the release of urine from the corresponding ureter will be delayed or not occur at all. In healthy pregnant women in the second half of pregnancy, there may also be a delay in the release of indigo carmine or even the absence of its discharge for 15 minutes due to atony and expansion of the ureter. · Cystoscopy. · Renal angiography, or nephrography, is an x-ray method of investigation in which a special contrast agent (diorast, cardiovascular) is injected through the femoral artery into the aorta at the level of discharge of the renal arteries using a special catheter. · Ophthalmologic examination of retinal vessels. · Radioisotope research (radioisotope nephrography) allows you to study the function of the kidneys. The patient is injected with intravenous substances labeled with I131, then using a multichannel radiographic unit, the function of each kidney is recorded separately (in the form of characteristic curves), the speed of blood purification from the labeled drug and its accumulation in the bladder. · Scintigraphy - a radioisotope study of the kidneys, carried out using a scintillation chamber. DIFFERENTIAL DIAGNOSTICSIt is very important to detect the presence of urinary tract infection. Pyelonephritis significantly worsens the prognosis of the disease and casts doubt on the possibility of a safe pregnancy. For diseases of the only kidney, pregnancy and childbirth are contraindicated. Pregnancy with nephrolithiasis of a single kidney is especially dangerous. Among the various complications in such cases was observed, in particular, excretory anuria, requiring emergency surgical intervention. Pregnancy is absolutely contraindicated in other diseases of a single kidney (tuberculosis, hydronephrosis, etc.), as well as in the presence of azotemia and hypertension. INDICATIONS TO CONSULTATION OF OTHER SPECIALISTSWith appropriate evidence, you may need to consult a general practitioner, urologist, nephrologist, TB specialist and an ophthalmologist. The observation of the pregnant woman is carried out in conjunction with the urologist. EXAMPLE OF FORMULATION OF DIAGNOSISPregnancy 33 weeks, headache presentation. The only kidney. Acute pyelonephritis in history. TREATMENTPREVENTION AND FORECASTING OF GESTATION COMPLICATIONSStarting from 4-6 weeks of pregnancy, women with a single kidney need careful urological and obstetric observation with periodic examination in the hospital. The absence of a kidney does not affect the duration of pregnancy. Symptoms of a threatened miscarriage occur in women with a history of obstetric and gynecological history (artificial or spontaneous abortions). At the same time, the kidney function is not impaired. Gestosis develops in women with a single kidney no more often than in a population. This fact is difficult to explain, but it undoubtedly has important practical significance. FEATURES OF TREATMENT COMPLICATIONS OF GESTATIONPrevention and prognosis of gestational complications For diseases of the only kidney, pregnancy and childbirth are contraindicated. Pregnancy is especially dangerous in case of nephrolithiasis of a single kidney, since severe complications can develop, in particular, excretory anuria, which requires urgent surgical intervention. Pregnancy is absolutely contraindicated in other diseases of a single kidney (tuberculosis, hydronephrosis, etc.), as well as in the presence of azotemia and hypertension. Treatment of complications of gestation on trimesters In the first trimester, there may be a threat of abortion, with traditional therapy being carried out. With the development of PN, delayed fetal development and chronic hypoxia in the second and third trimester, appropriate therapy is prescribed. In the third trimester, preeclampsia is being treated (onco-osmotherapy). With the threat of preterm labor, tocolytic therapy is used. Treatment of complications in childbirth and the postpartum period The prognosis for the mother and fetus is usually good if the pregnancy did not occur earlier than 1.5–2 years after nephrectomy or after surgery on a single kidney (removal of the stone, resection for tuberculosis), as well as in the absence during this period of time any disease in the remaining kidney. With CRF, the prognosis is uncertain. Such women should be carefully monitored throughout pregnancy and should be terminated immediately if the symptoms of renal failure are worsening. The prognosis for mother and fetus is undoubtedly unfavorable for the defeat or functional exhaustion of a single kidney. Such women are strictly forbidden to give birth, and if pregnancy occurs, it should be interrupted in the first 10–12 weeks. Treatment of urinary tract infections in women with one kidney is carried out according to the same principles as the treatment of pyelonephritis. In the absence of pyelonephritis, pregnant women who have undergone nephrectomy, as a rule, do not need treatment. The postpartum period proceeds safely. Obstetric complications (metroendometritis) and deterioration of the organs of the urinary system are rare and are not caused by previous nephrectomy. EVALUATION OF TREATMENT EFFICIENCYSELECTION OF TERM AND DECISION METHODBirths occur in a timely manner, with the exception of cases when they are called ahead of time due to the severity of the general condition of the patients. Delivery and cesarean section, usually proceed without complications. PATIENT INFORMATIONPregnancy is possible only with a satisfactory condition of a single kidney and the persistent desire of a woman to have children. · The term “single kidney” includes not only the congenital absence of a kidney, but also the loss of function of one of the kidneys as a result of a disease. · Pregnancy in women after nephrectomy, caused by kidney disease, usually proceeds normally. · Women with a single kidney need careful urological and obstetric observation starting at 4-6 weeks of pregnancy. Periodic examination is required in the hospital. · Treatment of urinary tract infections in women with one kidney should be carried out according to the same principles as treatment of pyelonephritis. In the absence of pyelonephritis, pregnant women who have undergone nephrectomy, as a rule, do not need treatment. |
| Read: |
|---|
Popular:
What is human blood
|
New
- Why do the pains of the fingers under the nails appear
- Determination of skin type and selection of cosmetics
- Summary of classes in fine arts in the older group with the use of non-traditional drawing techniques on the topic: Winter
- Materials for nail
- How to donate blood from a finger and why?
- Cheaper doesn't mean worse!
- Stages of inflammation
- What cough does a child give Ascoril?
- Mushroom like white but tubular
- Experiment: obtaining details of travel on the map "Plantain




